
 Tap to zoom
Tap to zoomComplete Guide to Prostate Cancer Screening: Steps and Results
Learn who needs prostate cancer screening, when to start based on age and risk, and how PSA, DRE, MRI, biomarkers, TRUS and biopsy guide diagnosis.
- Published on
- June 26, 2026
- Reading time
- 5 min read
- Last updated
- Updated: June 26, 2026
Prostate cancer screening means checking prostate health before pain or clear symptoms appear. This cancer often grows quietly without symptoms and may only become obvious after treatment has become more difficult.
The goal of screening is to find the disease earlier, when treatment decisions can be made more easily. Evaluation usually starts with a PSA test and a prostate examination, and if needed continues with more precise methods such as MRI and biopsy.
Urologic surgeon Prostate disease specialist
Note: To improve care quality and patient satisfaction, appointments are triaged by reason for visit. Each physician sees patients within the relevant urology subspecialty.
Book appointment
In this article, we explain the prostate cancer screening pathway step by step.
What Is Prostate Cancer Screening, and Why Is It Important?
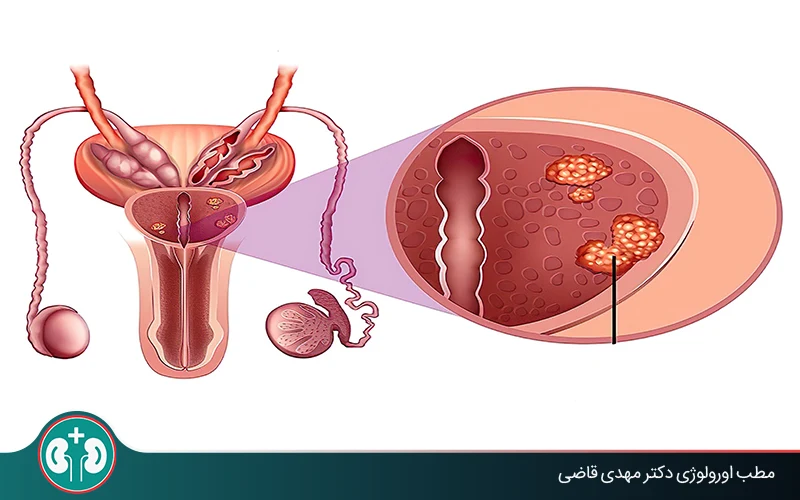
Prostate cancer is the second most common cancer in men. In many cases it begins without symptoms, or the symptoms are so mild that they are attributed to aging.
Fortunately, a set of tests and examinations called prostate cancer screening can help find the disease before serious urinary problems or pain appear. In other words, screening helps with prostate cancer diagnosis at an early stage, before it spreads or metastasizes to other organs.
Appointments related to Urologic surgeon Prostate disease specialist
Open the public booking path to review times and related information.
Book appointment
Screening can reduce the chance of death from prostate cancer because the disease has a high chance of successful treatment in its early stages. Timely diagnosis can also make prostate cancer easier to treat and manage with less invasive and less costly methods.

Who Needs Screening? People at Higher Risk
Not all men have the same risk of developing this disease. Some people have a higher chance because of genetic, medical, or environmental factors, so they need to start screening earlier and take it more seriously. If you are in one of the following groups, prostate cancer screening is especially important for you:
Genetics and Family History
Having prostate cancer in a first-degree relative, such as a father or brother, increases your risk. If the cancer was diagnosed at a younger age, the risk may be about twice as high.
Q&A — Urologic surgeon Prostate disease specialist
General questions are shown on the destination page after review.
Book appointment
Race (Black Men or Men of African Ancestry)
Prostate cancer is more common in Black men and often behaves more aggressively. This group has a higher risk not only of developing the disease, but also of faster progression and death from it.
Older Age
The risk of prostate cancer rises with age. From age 50 onward in particular, regular screening tests are worth discussing and performing as advised. The next section explains the age to start screening and the interval between tests in more detail.
Best Age to Start Prostate Cancer Screening
The starting age for prostate cancer screening is not the same for everyone; it is based on a person's risk level. The table below summarizes recommendations according to age and background risk factors.
Age | If you are in this group | Suggested action |
|---|---|---|
40 to 45 years | Prostate cancer in your father or brother / African ancestry | Start screening early |
45 to 50 years | No clear family history / average risk | Have the first baseline test |
50 to 69 years | All men | Regular screening every 2 to 4 years |
Older than 70 years | If life expectancy is less than 10 years | Stop routine screening |
At older ages, the chance of dying from prostate cancer is lower because the disease often progresses slowly in this age group. At the same time, cancer treatments can have significant side effects. For this reason, routine prostate cancer screening after age 70 is generally not recommended.
Main Screening Methods: Step One
In initial prostate cancer screening, decisions are not made from one number or one examination alone. That is why the first step usually uses two complementary methods: the PSA test and then a prostate examination through the rectum:
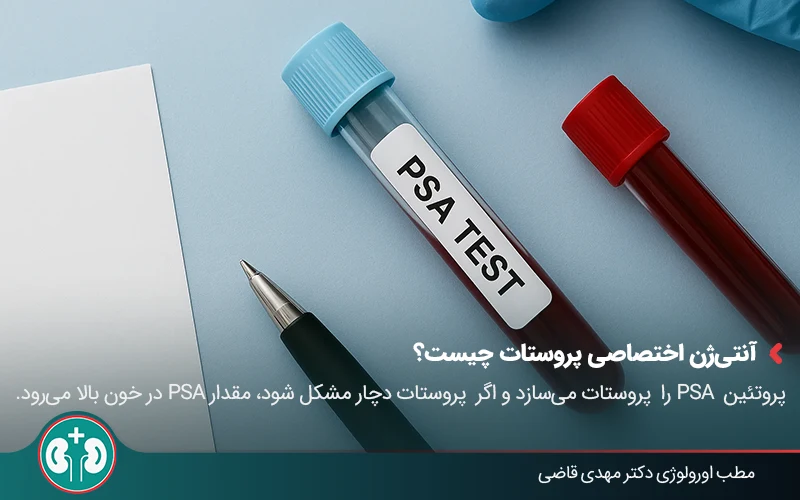
1. PSA Test (Prostate-Specific Antigen)
The PSA test is the first and main test used in prostate cancer screening. It is done with a blood test. PSA is a protein made by the prostate itself. When the prostate becomes larger, inflamed, or has abnormal changes, the PSA level in the blood can rise.
There is an important point to remember about prostate testing with PSA: there is no single number that proves PSA is definitely normal or definitely cancerous. Many men with a high PSA do not have cancer. Common problems such as benign prostatic hyperplasia, infection, or prostatitis can also raise the PSA level.
However, the doctor considers the following criteria for further evaluation:
A PSA above 4 needs further evaluation.
At younger ages, even a value above 2.5 may be important.
Note: these numbers are guides, not absolute cutoffs. The "PSA trend" and "individual risk" are more important.
Factors That Can Affect PSA Level and Screening Results
A urologist does not make a cancer decision based only on PSA. Some conditions can falsely raise or lower the PSA value. If these factors are not considered, the test result can be misleading.
Factors that can raise PSA:
Benign prostatic hyperplasia (BPH);
Urinary tract infection or prostatitis;
Ejaculation within 48 hours before the test;
Long-distance cycling;
Recent catheterization or prostate examination.
Factors that can lower PSA:
Use of medicines such as finasteride (for hair loss or prostate symptoms).
For this reason, tell your specialist about anything that may affect your PSA level. This simple information helps the prostate test be interpreted in the right clinical context.
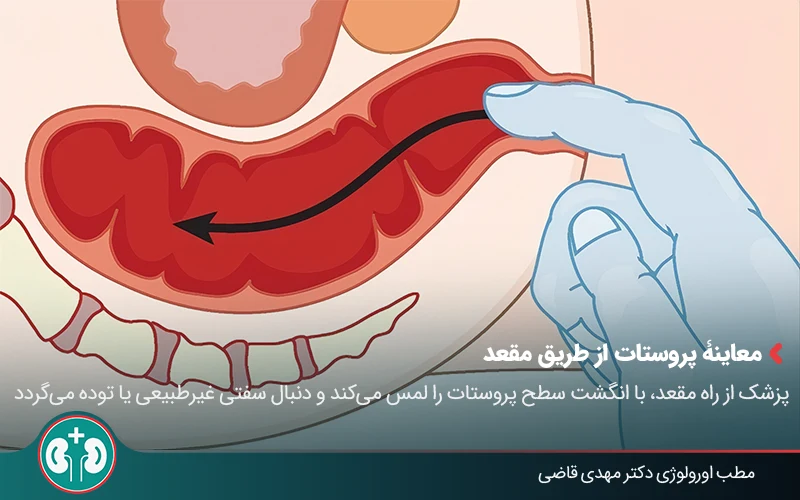
2. Prostate Examination Through the Rectum (DRE)
Along with the PSA test, digital rectal examination of the prostate is one of the two main methods in the first stage of prostate cancer screening. This examination allows the urologist to assess the prostate directly, not only through a blood-test number.
In this method, the doctor inserts a finger through the rectum to feel the surface of the prostate and look for abnormal hardness or a mass. A rectal prostate exam is usually very brief and not painful; most people feel only mild, temporary pressure.
The PSA value may be in the normal range, but the doctor may feel a lump or abnormal change during the prostate examination. For this reason, the finger exam complements the PSA test, and using both together gives the specialist a more accurate picture of prostate health.
What Happens If Screening Results Are Not Normal? Step Two
If the PSA test or prostate examination is not normal, you do not need to assume the worst right away. At this stage, before making a major decision, the doctor checks whether the PSA value is truly meaningfully elevated or has changed because of a temporary factor such as infection.
For this reason, the doctor may ask you to repeat the test after a period of time, or may start a short course of treatment such as antibiotics if there are signs of infection. If the PSA remains higher than expected after these checks, the doctor moves you to the next step, explained below step by step:
3. Additional Blood and Urine Tests (Biomarkers)
If PSA is mildly elevated and it is still unclear whether a biopsy is really needed, the doctor may order additional blood or urine tests to estimate the risk of prostate cancer more precisely.
These tests, called biomarkers, are used to estimate the likelihood of clinically significant cancer that needs treatment and to decide whether biopsy can be safely deferred for now.
If these tests show a low level of risk, the doctor may choose periodic follow-up and monitoring. If they show a higher level of risk, you will be referred to the next step: more detailed imaging.
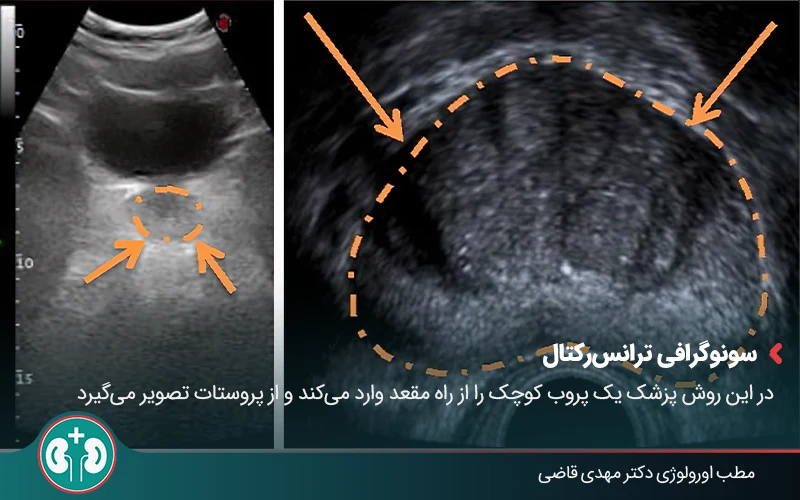
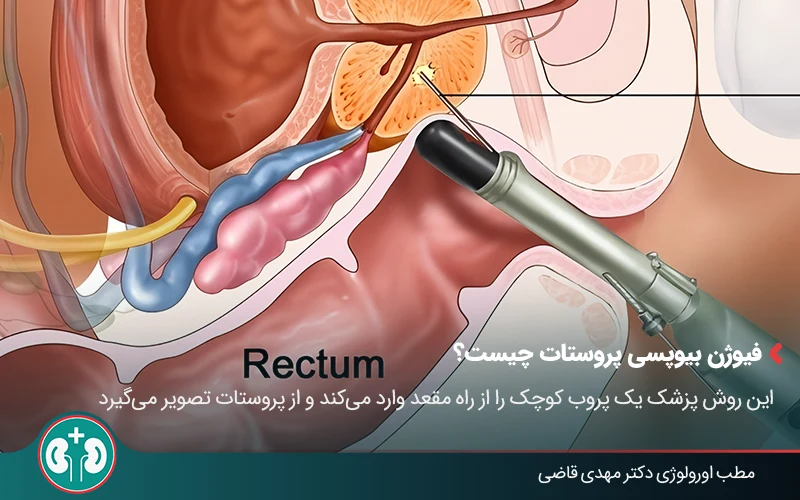
4. Transrectal Ultrasound (TRUS)
If it is still unclear after the previous checks whether you really need a biopsy, the urologist may use transrectal prostate ultrasound .
In this method, the doctor inserts a small probe through the rectum and creates images of the prostate. It takes a few minutes and is usually not painful; most people feel only some pressure.
Ultrasound alone is not the final basis for decision-making or a definitive cancer diagnosis, because it does not show many prostate cancers. The main role of transrectal ultrasound in screening is to guide the biopsy needle toward suspicious areas of the prostate; the biopsy section explains this in more detail.
5. Magnetic Resonance Imaging (MRI)
If, after all previous checks, the doctor is still not sure whether biopsy is necessary, prostate MRI may be done before taking tissue samples. The goal is to make sure that, if biopsy is needed, it is done for a sound reason and from the right area.
MRI helps the doctor see inside the prostate more clearly and determine whether there is an area suspicious for a cancerous lesion. The radiologist reviews the prostate MRI images and gives each area of the prostate a score from 1 to 5.
Result | Interpretation |
|---|---|
Score 1 to 2 | Low likelihood of cancer; biopsy not needed |
Score 3 | Borderline finding; needs more careful decision-making |
Score 4 to 5 | High likelihood of cancer; biopsy needed |
In this way, if a biopsy is needed for the final diagnosis of prostate cancer, MRI can identify the exact sampling site and improve diagnostic accuracy.
6. Prostate Biopsy
When previous evaluations show that the chance of cancer is significant, the doctor reaches the final and most important step: prostate biopsy. This is the only method that can say with certainty whether cancer is present.
During a biopsy, the doctor removes several very small pieces of prostate tissue with very thin needles. It is done with local anesthesia and is usually not painful; most people feel only brief pressure or discomfort.
After prostate biopsy, you may see a small amount of blood in the urine or semen for a few days. This is usually not a cause for concern and resolves on its own. The risk of infection is low, and the doctor usually gives antibiotics for prevention.
Prostate biopsy is performed by one of the following two methods.
Biopsy Guided by Transrectal Ultrasound
In this method, the doctor inserts a small probe through the rectum to view the prostate. The biopsy needle is then guided to suspicious areas with the help of that image, and samples are taken. This is the most common biopsy method.
Fusion Biopsy (More Precise Method)
In this method, the specialist matches previously obtained prostate MRI images with the live ultrasound image.
This helps the doctor place the biopsy needle exactly into the suspicious areas seen on MRI. For this reason, prostate fusion biopsy usually has higher accuracy than biopsy guided by transrectal ultrasound.
Interpreting Biopsy Results: Does Every Prostate Cancer Need Treatment?
Biopsy does not only show whether cancer is present; it also shows how aggressive the cancer is and how quickly it may progress. For this reason, biopsy results are reported as a Gleason Grade Group from 1 to 5.
Group 1 (Low Risk)
In this group, cancer cells grow slowly and usually do not pose an immediate threat to health. In most cases, the urologist chooses active surveillance: the disease is monitored with regular tests and examinations, and treatment starts only if the situation changes.
Group 2 and Higher
In these groups, the cancer behaves more aggressively and the chance of progression is higher. For this reason, the doctor may recommend active surveillance or a treatment intervention such as surgery or radiation therapy.
Final Word
Prostate cancer screening means checking prostate health before pain or serious symptoms appear. The process usually starts with a PSA test and examination, and if needed continues with MRI and biopsy.
The timing of screening is based on age and family history, but symptoms such as frequent urination, weak urine stream, or burning with urination need medical evaluation at any age.
If prostate cancer is diagnosed in its early stages, it is controllable and treatable in most cases.
Frequently Asked Questions
Actions & related links
Related articles
All articlesWhat Is Polycystic Kidney Disease? (Fetal and Adult PKD)
What is polycystic kidney disease? Learn about inherited ADPKD and ARPKD, fetal and adult symptoms, complications, diagnosis, medicines, surgery, diet, fluids, and prevention-focused care.
What Is a Renal Cortical Cyst? Symptoms, Diagnosis, and Treatment
Renal cortical cyst | Simple vs. complex kidney cysts | Warning symptoms | Diagnosis and treatment | Needle drainage, laparoscopy, medication, and ablation
Kidney Transplant: Cost, Blood Type Compatibility, and Surgical Method
What is kidney transplant? Learn about cost considerations, operation duration and method, diet, who may not be eligible, success rates, isolation precautions, and post-transplant care.
What Is Pyelonephritis? Kidney Infection Symptoms, Diagnosis, and Treatment
What is pyelonephritis? Learn kidney infection symptoms in women, children, men, and pregnancy; diagnosis, antibiotics, treatment, emergency warning signs, and cystitis differences.