
 Tap to zoom
Tap to zoomWhat Is Azoospermia? Causes, Diagnosis, and Treatment
Learn what azoospermia means, obstructive vs non-obstructive causes, diagnosis, sperm retrieval, and treatment options for male infertility.
- Published on
- June 26, 2026
- Reading time
- 5 min read
- Last updated
- Updated: June 27, 2026
Azoospermia, sometimes called a zero sperm count, is one of the major causes of male infertility. It means that no sperm are found in the semen. Blockage in the sperm transport pathway, hormonal problems, ejaculation disorders, and structural or functional problems of the testicles can all cause azoospermia. In this article, we review the types of azoospermia, its symptoms, treatment, and ways to reduce the risk of this condition.
What is azoospermia?
Azoospermia, or absence of sperm (Azoospermia), is a condition in which there is no sperm in the semen.
Men with this condition cannot cause pregnancy. Infertility is defined as the inability of a man to make his partner pregnant after 1 year of unprotected sex. This means that no birth-control method, such as pills, a diaphragm, condom, withdrawal, or rhythm method, has been used.
In these men, there is usually no visible change in the appearance of semen, because sperm make up only about 1 percent of semen volume. A diagnosis of azoospermia can be a major shock for a man. These men usually have normal sexual desire and sexual function; their problem is fertility only.
Symptoms of azoospermia
Inability to get a partner pregnant
Increased body fat, hair changes, or breast tissue
Watery, clear, or nearly white discharge from the penis
Varicocele; a lump or swelling on the scrotum that can feel like a bag of worms
Stress or emotional distress caused by inability to have a child
Small, soft, or non-palpable testicles
Large, twisted veins that may be seen in the scrotum (varicocele)
What causes azoospermia?
Among the obstructive causes of azoospermia are the following:
Trauma or injury to these areas
Infections
Inflammation
Previous pelvic surgery
Cyst formation
Vasectomy
Cystic fibrosis
Among the non-obstructive causes of azoospermia are the following:
Genetic causes such as Klinefelter syndrome, Kallmann syndrome, and Y-chromosome microdeletion
Hormonal imbalance and endocrine disorders, including hypogonadotropic hypogonadism, hyperprolactinemia, and androgen resistance
Ejaculatory problems such as retrograde ejaculation caused by medicines such as tamsulosin
Liver and kidney diseases
Testicular diseases such as mumps orchitis, testicular tumor, testicular torsion, undescended testicle, and absence of testicular development
Diabetes
Some causes of azoospermia are treatable, and treating them can preserve a man’s fertility potential.
What causes a zero sperm count?
Azoospermia may result from failure to produce sperm or from sperm being unable to reach the semen. Depending on laboratory findings, both factors may sometimes be present in one person. This problem has no symptoms that you can notice on your own, but if you have been trying to conceive for a long time and pregnancy has not occurred, azoospermia may be the cause.
Does azoospermia mean the testicles do not make sperm?
As noted above, azoospermia means that no sperm are found in the semen. However, azoospermia does not necessarily mean that the testicles do not make sperm. The more accurate meaning is that the testicle may be able to produce sperm, but a meaningful amount may not exit into the semen, so the spermiogram reports a zero sperm count.
Types of azoospermia
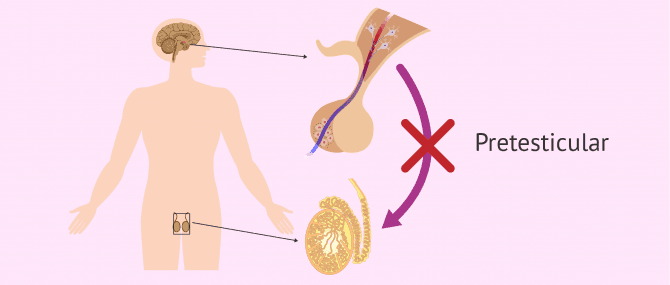
1. Pre-testicular azoospermia
This type affects about 2 percent of men with azoospermia and occurs because of disorders of the pituitary gland or hypothalamus. Sperm production in the testicles is controlled and stimulated by higher centers in the brain.
A hormone called FSH is secreted from a part of the brain called the pituitary gland and controls sperm production. If the pituitary gland does not secrete FSH for any reason, the person may develop a low sperm count and, in some cases, azoospermia. These patients can be treated by prescribing the required hormones. This type of azoospermia is uncommon and accounts for only 2 percent of all azoospermia cases.
2. Testicular azoospermia
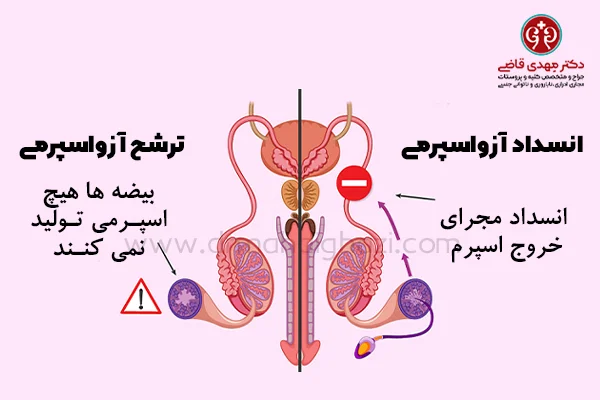
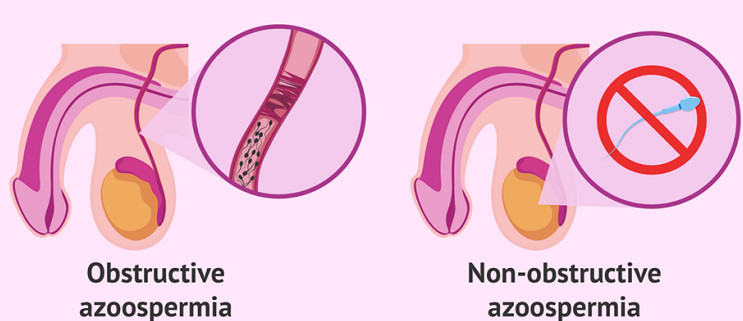
Testicular azoospermia, or non-obstructive azoospermia, affects about 49 to 93 percent of men with azoospermia. In men with non-obstructive azoospermia, there is reduced sperm production or no sperm production.
In these patients, the testicles are usually abnormal or small and sometimes may even be absent. Causes include undescended testicle, a history of infectious diseases such as mumps, genetic problems, and other factors. Azoospermia may also be seen after chemotherapy, radiotherapy, and similar treatments.
Azoospermia caused by testicular factors is the most common form of azoospermia and is sometimes called non-obstructive azoospermia. Until recent years, there was no specific treatment for these men, and the only options were donor sperm, donor embryo, or adoption. In recent years, however, microsurgical techniques have been used in the treatment of these men.
3. Post-testicular azoospermia
Post-testicular obstruction or retrograde ejaculation affects 7 to 51 percent of men with azoospermia. In this situation, sperm production exists, although the semen contains no sperm. If none of the above categories applies, we use the term idiopathic azoospermia (Idiopathic azoospermia).
In these patients, sperm are produced in the testicle, but a blockage in the ducts that carry sperm out of the testicle and into the semen prevents sperm from appearing in the semen. This type of azoospermia is seen in men who have had a vasectomy.
Another cause is congenital blockage in the sperm transport pathway. Because these men produce a suitable number of sperm, sperm can be used for in vitro fertilization after testicular sampling. In vasectomy cases, or in cases where previous surgery has blocked the ejaculatory ducts, reconstructive surgery may be used to reopen the pathway.
4. Idiopathic azoospermia
This is one of the most severe forms of male infertility and affects 1 percent of men. It has no clearly identified cause, but factors such as age and weight can influence it. For example, according to studies performed in 2013, obesity and excess weight are factors associated with oligospermia and azoospermia, although the main cause of the disorder remains unknown.
A severe form of male infertility that occurs without a clear cause is called “idiopathic azoospermia.” This disorder, which affects about 1 percent of men, can be worsened by obesity, excess weight, and increasing age.
Diagnosis of azoospermia
Hormone-level testing, physical examination, and medical history are used for the initial diagnosis of this condition. Childhood illness, family history, sexual dysfunction, testicular inflammation, a history of chemotherapy or radiotherapy, and any sexual injuries also affect the diagnostic process.
Physical examination also includes measuring the testicles, assessing testicular consistency, evaluating the epididymis, checking secondary sexual characteristics, and determining whether the person has varicocele. Hormonal evaluation includes serum testosterone and follicle-stimulating hormone levels.
Is azoospermia treatable?
Treatment for azoospermia depends on its cause. For each patient, the best treatment is chosen according to individual circumstances and based on many factors, such as the partner’s age, reproductive function, physical examination findings, blood-test results, and financial situation. Depending on the cause, many treatment options may be available. Azoospermia is treated with medication or surgery depending on its type:
- Treatment of obstructive azoospermia
In men with obstructive azoospermia, the following methods may be used depending on the patient’s condition:
1. Microsurgical connection of the vas deferens to the epididymis: This is an extremely difficult operation performed under a microscope and takes about three hours. Because the diameter of the vas deferens and epididymis is extremely small, the success rate is also low. In the hands of the best surgeons, sperm appear in the semen in about 25 percent of cases, but because sperm quality is low, the pregnancy rate is only 10 percent.
2. To reach the semen, sperm pass in order through the epididymis, the vas deferens, and the ejaculatory duct. Sometimes the blockage is in the ejaculatory duct. These patients are relatively easy to treat; the ejaculatory duct can be opened through the urethra with a simple incision.
3. In men with congenital bilateral absence of the vas deferens, a method called PESA is used. PESA stands for Percutaneous Epididymal Sperm Aspiration. In this procedure, sperm are obtained from the epididymis through the scrotal skin with a syringe, and fertilization is performed in the laboratory.
4. Another method is MESA. MESA stands for Microepididymal Sperm Aspiration. In this method, the scrotum is opened surgically, and the blocked portion of the epididymis is identified under the microscope (because dilation occurs behind the blockage). Sperm are aspirated with a syringe from the dilated area, the presence of sperm is confirmed under the microscope, and the sperm are used for fertilization in the laboratory.
5. Sometimes, in patients with obstructive azoospermia, sperm cannot be obtained from the epididymis. In these patients, TESA is used. TESA stands for Testicular Sperm Aspiration. In this procedure, sperm are aspirated from the testicle through the skin using special needles.
- Treatment of non-obstructive azoospermia
As noted, when the testicles do not produce sperm, this is called non-obstructive azoospermia. Testicular size and measurement of blood FSH help us quickly reach a likely diagnosis. If the testicles are small and the FSH level is high, the person most likely has non-obstructive azoospermia, and the chance of having a child is almost zero. Some men are born without the vas deferens. In these men, semen volume is extremely low, about half a milliliter.
In these men, testicular biopsy shows that the testicles do not produce sperm. These men are generally considered absolutely infertile, but in recent years there have been advances in this field. Non-obstructive azoospermia, or poor testicular function, has many causes. In some cases, sperm production by these testicles can be stimulated with medication. These cases include:
1. Men whose testicular size is normal and whose blood FSH level is not high may be able to stimulate sperm production with medication.
2. One cause of loss of testicular function is failure to operate on an undescended testicle at the right time. If this condition is bilateral, the man will become infertile. Some of these testicles can also be stimulated to produce sperm with medication.
3. Sometimes, in men with non-obstructive azoospermia, a small number of sperm are seen in testicular biopsy. The reason these men are azoospermic is that the sperm are lost during transport. Sperm obtained through biopsy can be used for fertilization in the laboratory.
4. Patients with non-obstructive azoospermia typically have small testicles, although in many cases the patient appears normal, the testicle is completely normal on examination, and semen volume and appearance are also normal. Hormonal testing is the basis of diagnostic evaluation. These patients need specialized hormonal assessment. A characteristic hormonal finding in men with non-obstructive azoospermia is a high FSH level.
Before any treatment, correctable problems in these patients, such as varicocele and hormonal disorders, should first be corrected, and the patient should avoid toxic exposures such as smoking. In addition to hormonal tests, genetic evaluation and Y-chromosome testing are also necessary.
5. Genetic testing
6. Men with non-obstructive azoospermia have a higher rate of genetic abnormalities than the general population. Every patient with azoospermia should undergo karyotype and Y-chromosome testing. Seventeen percent of men with non-obstructive azoospermia have genetic abnormalities.
7. Y-chromosome testing (AZF evaluation)
8. The Y chromosome is also called the male chromosome. Each chromosome has a short arm and a long arm. The end of the long arm of the Y chromosome contains several genes whose absence can cause azoospermia. One of these genes is called AZF. Abnormality in this gene region causes azoospermia.
Is azoospermia common?
According to available statistics, about 10 to 15 percent of couples are infertile. In 50 percent of cases, infertility is due to female factors, and in the other 50 percent it is due to male factors. About 10 percent of infertile men and 1 percent of all men have azoospermia. Semen analysis is the most important test for evaluating male fertility.
What methods are used to retrieve sperm?
In men with obstructive azoospermia, there are often many sperm in the reproductive structures, and several methods can be used to obtain sperm. These include testicular sperm extraction or testicular biopsy, testicular sperm aspiration, microsurgical epididymal sperm aspiration, and other techniques.
The choice of method differs according to each patient’s condition. For men with non-obstructive azoospermia, several approaches are available for treating male infertility, but the method most likely to find usable sperm for in vitro fertilization and intracytoplasmic sperm injection is microTESE, or testicular biopsy. This testicular biopsy involves careful incision through the testicular tubules to look for tissue that is likely actively producing sperm. This method allows the highest sperm yield while preserving as much of the other testicular tissue as possible, including the Leydig cells that produce testosterone.
Diseases associated with azoospermia
Hyperprolactinoma
Klinefelter syndrome
Orchitis
Testicular cancer
Cystic fibrosis
Ejaculatory duct obstruction
Retrograde ejaculation
Kallmann syndrome
Intellectual disability
Factors that affect azoospermia
Obesity
Excess weight
Pesticides
Drugs such as marijuana
Radiotherapy
Genital ulcers
Pelvic surgery
Antibiotic use

Ways to reduce the risk of azoospermia
Azoospermia is not always preventable, but by addressing some related factors, you may be able to reduce the chance of developing it. Weight loss and a healthy lifestyle are among the best options for reducing the risk of azoospermia. There is no way to prevent genetic diseases that cause azoospermia. To reduce the risk of azoospermia from non-genetic causes, the following steps can be recommended:
Avoid activities that carry a risk of injury to the reproductive system.
Avoid radiation exposure.
Know the possible side effects of your medicines.
Avoid exposing the testicles to high temperatures for long periods.
Final word
Receiving a diagnosis of azoospermia can be emotionally difficult. When this diagnosis is accompanied by other distressing information, such as a hereditary cause or the possibility of passing it to children, it can be even more upsetting. In this situation, it is best to seek help from a physician.
A physician can help you cope with the diagnosis and, at the same time, understand the options available to you. Some men may feel shame or embarrassment in this situation. If you experience these feelings, it is best to discuss them with your doctor.
Actions & related links
Related articles
All articlesWhat Is Polycystic Kidney Disease? (Fetal and Adult PKD)
What is polycystic kidney disease? Learn about inherited ADPKD and ARPKD, fetal and adult symptoms, complications, diagnosis, medicines, surgery, diet, fluids, and prevention-focused care.
What Is a Renal Cortical Cyst? Symptoms, Diagnosis, and Treatment
Renal cortical cyst | Simple vs. complex kidney cysts | Warning symptoms | Diagnosis and treatment | Needle drainage, laparoscopy, medication, and ablation
Kidney Transplant: Cost, Blood Type Compatibility, and Surgical Method
What is kidney transplant? Learn about cost considerations, operation duration and method, diet, who may not be eligible, success rates, isolation precautions, and post-transplant care.
What Is Pyelonephritis? Kidney Infection Symptoms, Diagnosis, and Treatment
What is pyelonephritis? Learn kidney infection symptoms in women, children, men, and pregnancy; diagnosis, antibiotics, treatment, emergency warning signs, and cystitis differences.
Comments
4 comments