
 Tap to zoom
Tap to zoomVesicoureteral Reflux (VUR): Urine Backflow From the Bladder to the Ureter
Learn about vesicoureteral reflux (VUR), urine backflow from the bladder toward the ureters and kidneys, including symptoms, causes, VCUG diagnosis, grading, follow-up, antibiotics, and surgery.
- Published on
- June 26, 2026
- Reading time
- 5 min read
- Last updated
- Updated: June 26, 2026
Most people are familiar with acid reflux, where stomach acid moves up and causes pain or a burning sensation in the chest area. But this is not the only type of reflux that occurs in the body, and the bladder can also experience reflux.
Bladder-ureteral reflux occurs when urine moves up instead of down. When urine flows backwards into the kidneys, it is called vesicoureteral reflux (VUR). If urine takes the wrong route to reach the kidneys, it can carry bacteria from the bladder to the kidneys and cause an infection.
If left untreated, kidney infections can lead to damage, scarring, and eventually long-term damage to the kidneys. About
1 in 100 newborns has vesicoureteral reflux (VUR). Family history and hereditary factors play a role in this.
How does the urinary system work?
The urinary system consists of two kidneys, two ureters, a bladder and a urethra.
The ureters carry urine from the kidneys to the bladder. These ureters are connected to the bladder by a one-way valve that allows urine to flow in only one direction, from the ureter to the bladder.
The bladder stores urine. One-way valves prevent urine from returning to the ureters.
Reflux may occur in one or both ureters. According to the severity of urine reflux, vesicoureteral reflux is divided into five grades, with grade five being the most severe. In severe reflux, the ureters and kidneys may
become enlarged and twisted; More severe reflux is associated with a greater risk of kidney damage if there is an infection. Vesicoureteral reflux (VUR) is often asymptomatic, meaning it usually does not cause pain or urinary symptoms.
Bladder-ureteral reflux symptoms
Symptoms of vesicoureteral reflux (return of urine) may be observed even before the birth of the child; But it is mostly
diagnosed when the child has frequent urinary infections. Many patients with mild reflux may be asymptomatic for years. This disease is
rare in older children and adults and is more common in girls. Possible symptoms of bladder-ureteral reflux that should be considered:
Pain or burning when urinating
A frequent need to urinate, even if there is only a small amount of urine
Unexplained fever
Pain in the abdomen or side
Bad smell of urine
Bedwetting in older children
Necessity of treatment of bladder-ureteral reflux
Treatment of vesicoureteral reflux (VUR) depends on the child's symptoms. The good news is that most children will get over it without surgery and will have no problems. In mild cases, regular monitoring of the child's condition is sufficient, and sometimes mild antibiotics are used to prevent urinary tract infections.
But if children suffer from frequent and severe kidney infections due to bladder to ureter reflux, this disease is more serious and in such
cases, anti-reflux surgery may be necessary. Surgery can help prevent further damage to the kidneys and improve the quality of life of the child.
Bladder-ureteral reflux can improve over time and as the child grows. Careful follow-up and appropriate treatment can help prevent serious complications and improve the child's condition.
Causes of urine reflux
Backflow of urine, or vesicoureteral reflux (VUR), is usually caused by a congenital defect in the ureteral valve in the bladder. This defect in the formation and function of the valve leads to its inefficiency and the urine returns upwards instead of downwards.
The ureteral valve, which normally functions as a one-way valve. It should direct the urine from the ureter to the bladder and prevent its return, and if this valve is defective, this function will be impaired and the urine can return to the kidneys.
The main cause of this birth defect is not fully known; But genetic factors can play a role in it.
In other words, if one of the child's parents or siblings has vesicoureteral reflux, the child is more likely to develop it, and in addition, male babies born with other birth defects may be at greater risk. In some cases, the cause of urine reflux is not completely emptying the bladder.
This is less common but can lead to reflux. When the bladder does not empty completely, residual urine in the bladder may put more pressure on the ureter, causing urine to back up into the kidneys. This condition can be caused by nerve disorders, urethral obstructions, or functional disorders of the bladder. These factors can lead to increased pressure in the bladder and ureters and cause urine to return to the kidneys.
Although bladder-ureteral reflux is often detected after the diagnosis and treatment of a urinary infection in a child, it should be noted that bladder-ureteral reflux itself does not cause a urinary infection, and a urinary infection does not lead to reflux.
However, the presence of reflux can increase the risk of urinary tract infections; When the urine returns to the kidneys, the bacteria in the bladder may reach the kidneys along with the urine and cause an infection. Frequent kidney infections can lead to serious and permanent kidney damage.
Finally, accurate diagnosis of the cause of urine reflux requires careful medical examinations and tests; Imaging methods such as ultrasound, voiding cystography (VCUG), and nuclear scans can help identify and diagnose structural and functional defects in the urinary tract.
Based on the results of these tests, the doctor can determine the best treatment method for the child.
Bladder-ureteral reflux diagnosis
Diagnosing bladder-ureteral reflux requires history and specialized paramedical examinations to confirm the diagnosis
Answers to the following questions can help doctors diagnose and manage vesicoureteral reflux (VUR):
Does the child urinate regularly?
Checking the regularity of the child's urination times can indicate the correct functioning of the bladder.
Does the child have normal urinary control during the day?
Normal urinary control during the day can be a sign of healthy functioning of the urinary system.
Does the child empty his bladder completely?
It is very important to empty the bladder completely, because urine remaining in the bladder can lead to urinary infections and exacerbation of reflux.
Is the child constipated?
Constipation can put more pressure on the bladder and cause problems with passing urine, which can exacerbate reflux.
Paramedical methods of diagnosing bladder-ureteral reflux
Prenatal ultrasound
Sometimes symptoms of vesicoureteral reflux (VUR) can be seen prenatally using ultrasound. This method can detect early signs of disorders in the urinary system.
Urinary cysto-urethrogram(VCUG)
Bladder-ureteral reflux is usually diagnosed with a special imaging test called a voiding cysto-ureterogram (VCUG). This is an X-ray imaging method of the bladder and includes the following steps:
Inserting a catheter into the urethra.
Entering the contrast material through the catheter into the bladder until the bladder is full.
The child is asked to urinate.
Imaging of the bladder to check if contrast material has returned up toward one or both kidneys.
This test takes about 15 to 20 minutes and helps doctors determine the extent and degree of reflux.
Nuclear scan of the bladder
Another method to detect vesicoureteral reflux is to use a small amount of radioactive material in the liquid that enters the bladder through a catheter. Using a special camera, the radioactive material is tracked and the returned urine is shown in the images. This method is known as bladder nuclear scan and is highly accurate in diagnosing reflux.
Bubble ultrasound
Another method is to use bubbly liquid in the bladder and ultrasound to diagnose reflux; This method is non-invasive and can provide accurate information about the presence and severity of reflux. Since one of the risks of any diagnostic test is the possibility of infection due to the use of the catheter, the urologist may prescribe antibiotics before and after the test. This action helps to prevent infections caused by the entry of bacteria through the tube.
Additional tests
If vesicoureteral reflux is diagnosed, additional imaging tests may be needed to check kidney function and assess possible damage. These tests can include kidney and bladder ultrasound to check the size and growth of the kidneys.
These tests help doctors to assess the extent of kidney damage and determine the appropriate treatment plan.
Finally, accurate and timely diagnosis of vesicoureteral reflux can prevent more serious problems such as permanent kidney damage. Therefore, the use of appropriate diagnostic methods and regular follow-up of the patient's condition is of great importance.
Grading of vesicoureteral reflux
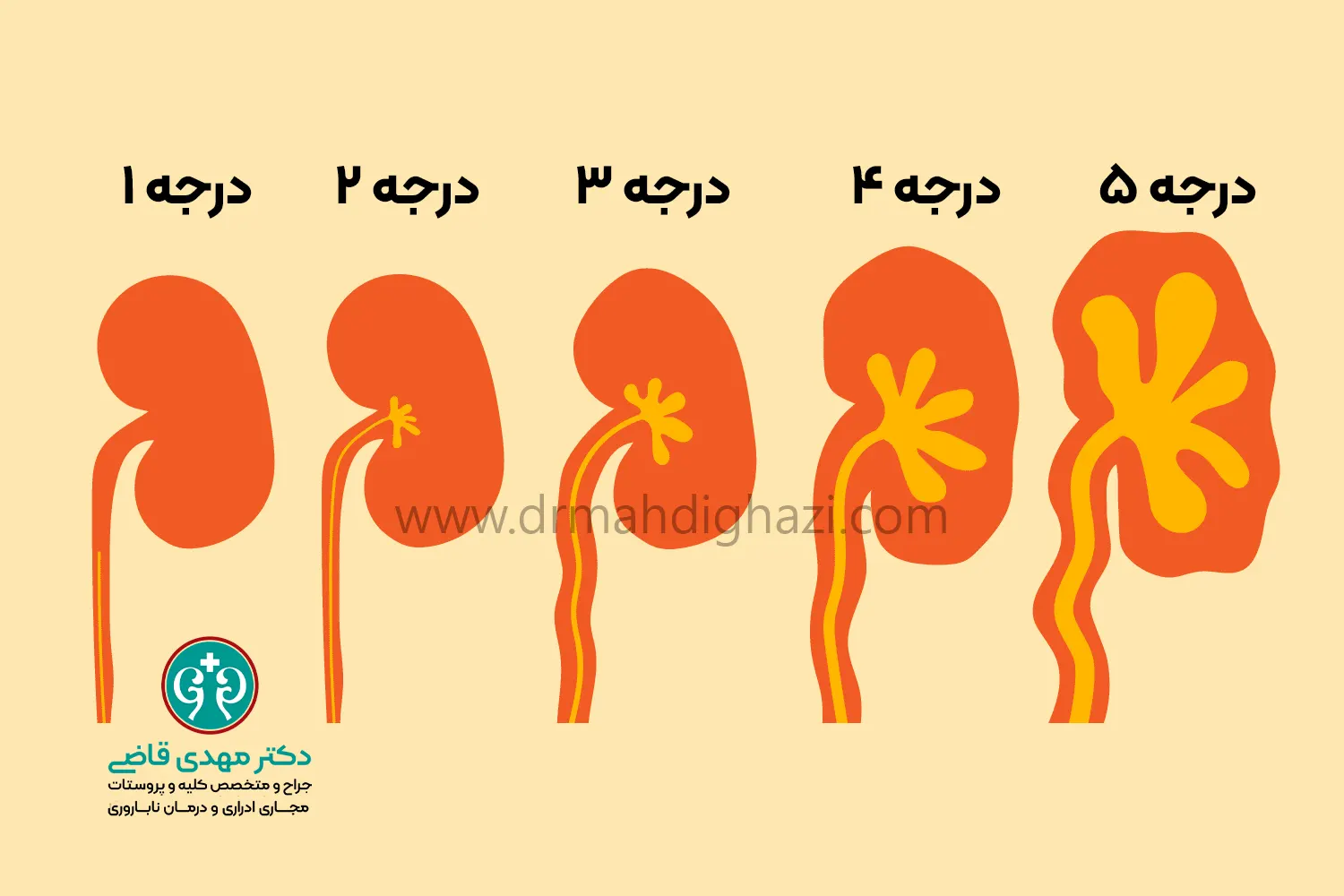
Grading of bladder-ureteral reflux plays an important role in the diagnosis and management of this disease; This system helps doctors to choose appropriate treatment methods to prevent kidney damage and improve the patient's quality of life by evaluating the severity of reflux. Regular follow-up and timely treatment can minimize the risks of vesicoureteral reflux and prevent more serious problems.
Bladder-ureteral reflux (VUR) is typically divided into five different grades using the International Classification System. This system helps doctors determine the severity of reflux and the need for treatment.
GradeI:
Urine returns only to the ureter and does not reach the kidney.
This grade of reflux is the mildest and rarely causes kidney damage.
GradeII:
The return of urine also reaches the kidney, but it does not cause swelling of the kidney.
In this degree, urine reaches the urine collection system in the kidney, but the structure of the kidney is still normal and no hydronephrosis is observed.
GradeIII:
Backflow of urine in the kidney has caused swelling and mild hydronephrosis.
This degree indicates the partial swelling of the kidney, which occurs due to increased urine pressure. The urine collection tubes in the kidney may be slightly dilated.
GradeIV:
There is moderate dilatation or hydronephrosis in the kidney.
At this stage, the swelling of the kidney increases and the ureters also dilate. This degree of reflux carries a higher risk of kidney damage.
GradeV:
Reflux leads to severe hydronephrosis and obvious torsion of the ureter.
This degree is the most severe type of reflux, which causes severe swelling of the kidney and twisting of the ureters, the internal structures of the kidney are severely affected, and this condition can lead to serious and permanent kidney damage.
Bladder-ureteral reflux grading is usually done through voiding cysto-ureterogram (VCUG) or other imaging methods such as ultrasound and nuclear scan. This grading helps doctors to choose the best treatment method.
Factors affecting thegrading of reflux:
Age of the patient: Reflux is morecommon in babies and young children andmay change as the child grows.
Severity of symptoms: Some children with low degrees of reflux mayhave no symptoms, while with higher degrees, more symptoms are observed.
History of urinary tract infections: Children with frequent urinarytract infections may have higher degrees of reflux.
Importance oftreatment:
Low grades I and II regular follow-up and sometimes theuse of prophylactic antibiotics.
Intermediate grades IIIand IV mayrequire more carefulfollow-up and medical oreven surgical interventions.
Grade: V often requires surgery tocorrect the ureteral valve defect andprevent further damage to the kidney.
Treatment options may include antibiotic medications to prevent infection, regular follow-up, and, if necessary, surgery to correct the ureteral valve defect.
vesicoureteral reflux treatment
Non-surgical treatment
Mild reflux often resolves with time and the normal function of the valve between the bladder and the ureter. With age, this valve becomes more efficient, and as a result, the possibility of reflux increases. Less severe reflux has a better chance of getting better on its own, and the average age at which this happens is five to six years.
The goal of medical or non-surgical treatment is to prevent urinary tract infections and kidney damage during the child's growth.
Inefficient bladder excretion syndrome and bladder to ureter reflux
Some children with vesicoureteral reflux may have this problem due to having "dysfunctional voiding syndrome" or "dysfunctional urinary excretion". This condition occurs when the child rarely goes to the bathroom or does not empty his urine completely. This can be due to incorrect urinary habits or neuromuscular problems.
Risks associatedwith bladderdysfunction syndrome:
Kidney infections: Children with irritable bowel syndrome are atincreased risk for kidney infections if they have reflux.These infections can cause serious damage to the kidneys.
Pressure on the bladder and ureters: Incomplete emptyingof the bladder can put more pressure onthe bladder and ureters and aggravate reflux.
Management and treatment of dysfunctional bladder voiding syndrome and vesicoureteral reflux
Training andbehavior modification:
Teaching the child: Teaching children toregularly go to the bathroom and emptythe bladder completely can be helpful.
Good hygiene habits: Teaching good hygiene habits, such asdrinking enough water and using the toilet regularly, can helpreduce the risk of reflux and urinary tract infections.
Use ofmedicine:
Antibiotics: In cases where the childgets frequent urinary infections, the useof preventive antibiotics can be effective.
Bladder control medications: In somecases, medications that help controlbladder function can be helpful.
Regular medicalfollow-up:
Regular check-ups: Regular follow-up with a urologistis necessary to evaluate the progress oftreatment and the condition of the kidneys.
Imaging tests: If necessary, imaging testsare useful to assess the severityof reflux and kidney damage.
The diagnosis and treatment of these patients requires careful examination and answers to key questions about the child's urinary habits. Propermanagement of this problem can prevent frequent infections and serious damage to the kidneys. The use of educational methods, medication andregular medical follow-ups can help improve the quality of life of children with inefficient bladder excretion syndrome and bladder-ureteral reflux.
In non-surgical treatment, the child periodically visits the doctor's office for examination.
In these examinations, urine and blood tests are performed to check urinary infection and kidney function. Bladder and/or kidney ultrasound and cysto-ureterurogram (VCUG) are also performed to check the condition of reflux and kidney development.
Surgical treatment
The goal of surgery is to treat reflux and prevent the dangers of reflux. Surgery is often performed under general anesthesia.
open surgery
In open surgery, the surgeon makes a small incision in the lower abdomen and repairs the connection between the one-way valve of the ureter and the bladder. This surgery can also be performed using robotic or laparoscopic surgery. This surgery is done in several ways and no synthetic material is used in them and finally they have a very good treatment response.
Injection of anti-reflux substances into the bladder
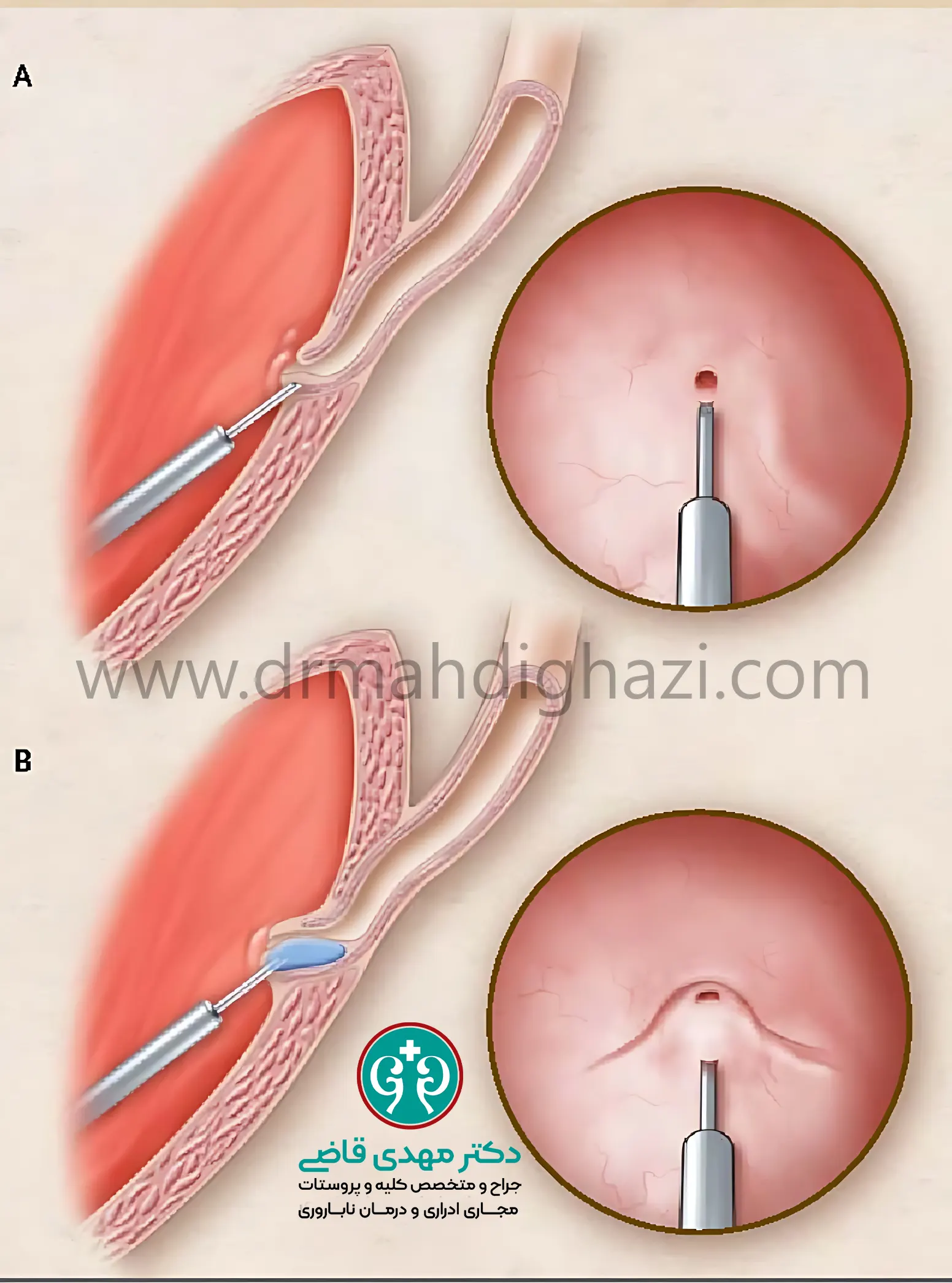
In endoscopic injection of anti-reflux substances, the surgeon inserts an instrument called a cystoscope through the urethra into the bladder to see the inside of the bladder. Then a substance is injected into the area where the ureter enters the bladder to narrow the opening of the ureter and prevent the return of urine. This procedure requires general anesthesia and in most cases can be done on an outpatient basis and does not require cutting or razor. The success rate of this method compared to conventional surgery depends on the condition of the patient's urethra. If surgery is needed, the urologist will discuss the various options with the family along with the complications and benefits of each.
After surgery
After surgery, the patient is generally hospitalized for one to two nights. During this time, a catheter is often used to empty the bladder.
A few months after surgery, an ultrasound and/or cystoureterogram (VCUG) is performed to ensure the procedure was successful. Once the reflux is corrected, the problem will most likely not return.
After treatment for vesicoureteral reflux, the child should feel better.
The urologist may prescribe periodic examinations to make sure that the healing process is progressing well and that there are no problems.
It is important to prevent future UTIs or treat them quickly to maintain good health. Prompt treatment of infections can reduce the risk of kidney ulcers.
Some urologists may recommend that baby boys be circumcised to prevent infections.
In the post-surgery care period, some doctors suggest using low-dose, long-term antibiotics to prevent urinary tract infections. This recommendation is usually based on the child's history of infections and bladder health.
Another option is to use high-dose antibiotics when an infection occurs. Some studies suggest that antibiotics may lead to an increased risk of health problems in adulthood. Also, antibiotics can cause the body to lose beneficial bacteria that are essential for good health.
Parents should consult their doctor to choose the best prevention option.
Frequently asked questions
Actions & related links
Related articles
All articlesWhat Is Polycystic Kidney Disease? (Fetal and Adult PKD)
What is polycystic kidney disease? Learn about inherited ADPKD and ARPKD, fetal and adult symptoms, complications, diagnosis, medicines, surgery, diet, fluids, and prevention-focused care.
What Is a Renal Cortical Cyst? Symptoms, Diagnosis, and Treatment
Renal cortical cyst | Simple vs. complex kidney cysts | Warning symptoms | Diagnosis and treatment | Needle drainage, laparoscopy, medication, and ablation
Kidney Transplant: Cost, Blood Type Compatibility, and Surgical Method
What is kidney transplant? Learn about cost considerations, operation duration and method, diet, who may not be eligible, success rates, isolation precautions, and post-transplant care.
What Is Pyelonephritis? Kidney Infection Symptoms, Diagnosis, and Treatment
What is pyelonephritis? Learn kidney infection symptoms in women, children, men, and pregnancy; diagnosis, antibiotics, treatment, emergency warning signs, and cystitis differences.
Comments
0 comments
No comments yet. Be the first to share your thoughts.