
 Tap to zoom
Tap to zoomWhat Is Ureteropelvic Junction Obstruction (UPJO)?
Learn about ureteropelvic junction obstruction (UPJO), including causes, symptoms, diagnosis, surgery, follow-up care, and kidney health.
- Published on
- June 26, 2026
- Reading time
- 5 min read
- Last updated
- Updated: June 27, 2026
Kidneys produce urine by filtering blood and removing waste products, salt, and water. Urine drains from the kidney into the renal pelvis and then into the ureter. Each kidney needs at least one functioning ureter to carry urine from the kidney to the bladder.
Ureteropelvic junction obstruction (UPJO) is a condition in which the kidney outlet, called the renal pelvis, is partially or completely blocked. The renal pelvis is the point where the kidney connects to the ureter; the ureters are tubes that carry urine to the bladder.
Urologic surgeon Kidney stone and urinary tract specialist
Note: To improve care quality and patient satisfaction, appointments are triaged by reason for visit. Each physician sees patients within the relevant urology subspecialty.
Book appointment
This condition can lead to dilation of the renal pelvis and kidney damage because urine cannot leave the kidney normally and collects inside it.
Obstruction at the renal pelvis can increase pressure inside the kidney and, as a result, cause kidney injury and dilation.
In some cases, surgery is needed to improve urine flow. This surgery may involve removing part of the renal pelvis, or creating a new urinary drainage pathway surgically to improve urine flow. In milder cases, when the obstruction is not severe enough to require urgent surgery, periodic monitoring may be enough.
Appointments related to Urologic surgeon Kidney stone and urinary tract specialist
Open the public booking path to review times and related information.
Book appointment
Causes of UPJO
Ureteropelvic junction obstruction (UPJO) is often congenital, and its cause is unknown. About 1 in every 1,500 children is born with this problem. The obstruction develops while the kidney is forming during fetal life. Today, most cases are diagnosed before birth with ultrasound. In adults, narrowing may occur after an impacted kidney stone, surgery, inflammation, or masses in the upper ureter.
Congenital Causes
In congenital cases, a defect in the normal development of the ureteropelvic junction can lead to narrowing. This defect may be due to abnormal development of the ureteral muscles or vascular abnormalities that compress the ureteropelvic junction.
Acquired Causes
In acquired cases, factors such as trauma, chronic inflammation, previous surgery, and kidney stone formation can cause narrowing at the ureteropelvic junction. These conditions can create scar tissue (fibrosis) and obstruct the urinary tract.
Q&A — Urologic surgeon Kidney stone and urinary tract specialist
General questions are shown on the destination page after review.
Book appointment
Symptoms
After birth, signs and symptoms in infants and children include:
Abdominal mass
Urinary tract infection with fever
Flank pain (pain in the upper abdomen or back, mainly after fluid intake)
Kidney stones
Vomiting
Poor growth in infants
In some cases, ureteropelvic junction obstruction (UPJO) has no obvious symptoms. Urine may drain normally at times, while at other times the pathway becomes blocked and causes intermittent pain.
The general view is that most children do not experience pain unless they develop a urinary tract infection or the obstruction becomes more severe.
Symptoms in Infants and Children
In infants, there may be a palpable mass in the abdomen, indicating kidney swelling. Recurrent urinary tract infections and fevers with no clear cause can also be important signs. In more severe cases, the infant may have feeding problems and poor growth.
Symptoms in Adults
In adults, symptoms may include severe flank pain that radiates to the lower abdomen or groin. This pain usually worsens after drinking a large amount of fluids or alcohol. Kidney stones and blood in the urine are also common symptoms in adults.
Diagnostic Methods
Although ultrasound helps the physician view the kidneys, additional imaging is needed to confirm ureteropelvic junction obstruction.
For an accurate diagnosis, the urologist needs to assess urine production and drainage.
Several tests are available for this purpose, and BUN and creatinine tests are used to evaluate kidney function.
In the past, intravenous pyelography, or IVP, was often used.
Nuclear renal scan and CT scan are also used for diagnosis.
Magnetic resonance imaging (MRI) may also be used.

Ultrasound
Ultrasound is one of the main methods for diagnosing ureteropelvic junction obstruction. It is noninvasive and painless and can provide detailed images of the kidneys and urinary tract. Ultrasound can show kidney swelling (hydronephrosis) and obstruction in the urinary tract.
Intravenous Pyelogram (IVP)
Intravenous pyelography is an imaging method that uses X-rays and contrast material to evaluate urine flow from the kidneys to the bladder. It can show the location and severity of the obstruction well. In this test, contrast material is injected into the bloodstream, and X-rays show the contrast entering the kidney and being excreted in the urine.
Nuclear Renal Scan
In this method, radioactive material is injected into the body and images of kidney function are obtained. A nuclear renal scan can show how the kidneys filter urine and how urine flows from the kidneys into the ureters and bladder.
CT Scan and MRI
These high-resolution imaging methods can provide detailed images of the kidneys and urinary tract. CT scan and MRI can show structural abnormalities and urinary tract obstructions in greater detail, but MRI is expensive and not available everywhere.
UPJO Treatment
Not all cases require treatment, and specialists have different opinions on this topic. Poor urine drainage in infants and children under 18 months may be temporary.
Many infants with good kidney function and poor urine drainage improve after a few months. However, in some infants the obstruction does not improve or even gets worse, making surgery necessary.
Adults with severe obstruction or complications such as kidney stones, urinary tract infection, or reduced kidney function may need surgery.
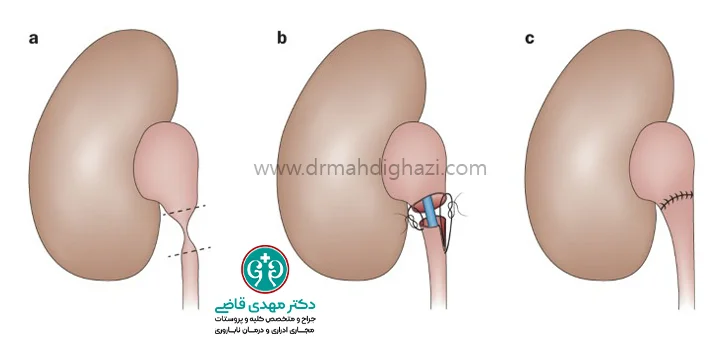
Open Pyeloplasty
The classic treatment for infants is pyeloplasty. In this operation, the narrowed part of the junction between the renal pelvis and ureter is removed, and the ureter is reconnected to the renal pelvis after creating a wide opening.
This process allows urine to drain quickly and easily and reduces the patient's symptoms and risk of urinary tract infection.
The surgeon's incision is usually 2 to 3 inches long and is placed just below the ribs. This surgery usually takes several hours and has a high success rate (95% success).
The patient may stay in the hospital for one or two days after surgery.
Ureteral stents may be used to speed recovery.
Minimally Invasive Surgery
Newer surgical options are less invasive:
Laparoscopic Pyeloplasty: This surgery may be performed with or without robotic assistance. In this method, the surgeon operates through two or three small openings in the abdominal wall using laparoscopic instruments. Benefits include less pain and nausea and a smaller scar, especially in older children and adults.
Endopyelotomy at the Narrowed UPJ: In this method, under camera guidance and with a special instrument, a wire is passed through the urethra and bladder into the ureter. The wire is used to cut the narrowed UPJ from the inside. A special ureteral stent remains in place for several weeks and is then removed. With this method, the UPJ heals in a wider shape, but repeat surgery may be needed. The success rate is lower than with open or minimally invasive surgery, but its benefits also include less pain and nausea.
Care After Treatment
Patients usually recover quickly. After surgery, the ureter may remain swollen for a while. Some patients have pain for a few days after surgery. Urine drainage from the kidney often improves as swelling in the operative area resolves. The physician uses ultrasound a few weeks after surgery to check for hydronephrosis. Sometimes, to help the kidney drain properly during healing, a ureteral stent is left in place for several weeks to several months. The kidney's appearance improves over time, although it does not return completely to normal.
Follow-Up and Monitoring
After surgery, regular follow-up with the physician is necessary to check the kidneys and ensure complete recovery. The physician may order imaging tests such as ultrasound and nuclear renal scan to evaluate kidney function and make sure there is no recurrent obstruction. Periodic blood tests may also be needed to check kidney function and ensure that no side effects have developed.
The kidneys may still contain some collected urine even if overall urine drainage has improved, and they may be slightly more prone to stones or infection in the future.
Sometimes a child who had partial obstruction in infancy that resolved naturally later develops signs of obstruction and needs surgery.
Preventing Complications
Special care is needed to prevent complications caused by ureteropelvic junction obstruction:
Adequate Fluid Intake: Adequate fluid intake can help prevent kidney stone formation and improve urine flow.
Healthy Diet: A balanced, low-salt diet can help maintain kidney health and reduce the risk of high blood pressure.
Preventing urinary tract infections: Good hygiene and seeing a physician if urinary tract infection symptoms occur can help prevent recurrent infections.
Regular Medical Follow-Up: Regular medical visits and periodic tests can help identify and treat any problem promptly.
Summary
Ureteropelvic junction obstruction is an important abnormality that can cause serious problems with kidney function. Early diagnosis and appropriate treatment can prevent permanent kidney damage. With modern surgical methods and postoperative care, many patients can recover fully and return to normal life.
Frequently Asked Questions
Actions & related links
Related articles
All articlesWhat Is Polycystic Kidney Disease? (Fetal and Adult PKD)
What is polycystic kidney disease? Learn about inherited ADPKD and ARPKD, fetal and adult symptoms, complications, diagnosis, medicines, surgery, diet, fluids, and prevention-focused care.
What Is a Renal Cortical Cyst? Symptoms, Diagnosis, and Treatment
Renal cortical cyst | Simple vs. complex kidney cysts | Warning symptoms | Diagnosis and treatment | Needle drainage, laparoscopy, medication, and ablation
Kidney Transplant: Cost, Blood Type Compatibility, and Surgical Method
What is kidney transplant? Learn about cost considerations, operation duration and method, diet, who may not be eligible, success rates, isolation precautions, and post-transplant care.
What Is Pyelonephritis? Kidney Infection Symptoms, Diagnosis, and Treatment
What is pyelonephritis? Learn kidney infection symptoms in women, children, men, and pregnancy; diagnosis, antibiotics, treatment, emergency warning signs, and cystitis differences.