
 Tap to zoom
Tap to zoomBladder Prolapse Surgery: Laparoscopic, Vaginal, and Open Repair
Bladder prolapse surgery for urinary leakage and pelvic heaviness: recovery, risks, laparoscopic, vaginal, and open approaches, steps, and aftercare.
- Published on
- June 26, 2026
- Reading time
- 5 min read
- Last updated
- Updated: June 27, 2026
Bladder prolapse is a condition in which the muscles and tissues that support the bladder become weak and the bladder drops toward the vagina. Signs of bladder prolapse include a feeling of heaviness or pressure in the pelvis or vagina, urinary incontinence, and a sensation of a lump or bulge in the vagina. Many women from middle age onward experience this disorder. One treatment method is bladder prolapse surgery using laparoscopy.
In this article, we discuss laparoscopic bladder prolapse surgery and provide complete details about this effective, minimally invasive method. Stay with us to the end for comprehensive, specialized information about this effective treatment.
What is bladder prolapse or cystocele, and why does it occur?
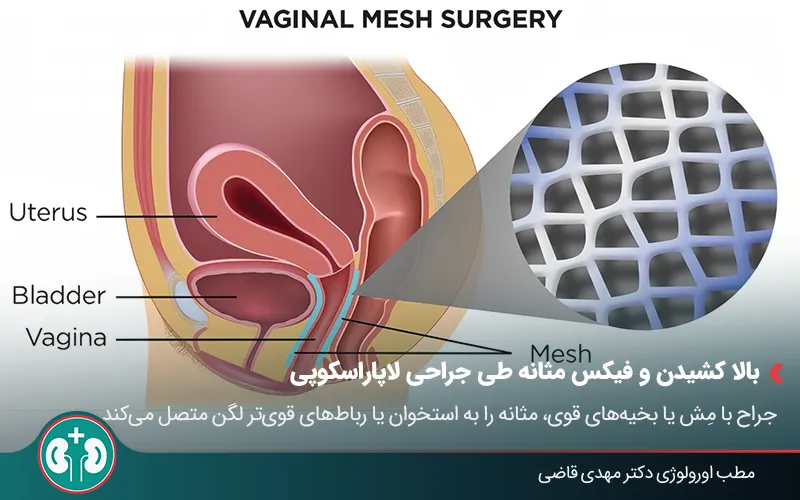
Bladder prolapse, or bladder prolapse, medically called cystocele, is a disorder in which the bladder drops from its normal position in the pelvis and presses on the front (anterior) wall of the vagina; therefore, this problem is also called anterior vaginal prolapse.
The bladder is held in place by a network of strong muscles and connective tissues called the pelvic floor muscles. These muscles act like a supportive mesh.
When these muscles and connective tissues become weak and loose because of pressure or injury, they can no longer hold the bladder firmly. As a result, under the force of gravity and internal body pressure, the bladder moves downward and into the vagina.
Causes and predisposing factors for bladder prolapse
Bladder prolapse, or cystocele, is usually the result of a combination of factors that weaken the supportive structures of the pelvic floor:
Vaginal delivery: pressure and stretching of tissues during difficult or multiple deliveries;
Menopause and reduced estrogen: reduced estrogen causes thinning and weakening of pelvic tissue;
Chronic pressure: repeated activities such as lifting heavy objects, straining during constipation, or chronic coughing;
Obesity and low physical activity: long-term pressure on the pelvic-floor muscles and ligaments;
History of pelvic surgery or hysterectomy: possible injury to pelvic supportive tissues;
Connective tissue disorders or genetic factors: congenital or inherited weakness in the structures that support the bladder.
Keep in mind that bladder prolapse is not a sign of personal weakness or negligence. This condition is a natural process in the body that often occurs because of hormonal changes and the physical pressures of life.
Different grades of bladder prolapse severity | ||
|---|---|---|
Severity grade | Condition | Possible symptoms |
Mild | The bladder has descended slightly toward the vagina (above the vaginal opening) | It may be asymptomatic or accompanied by a slight feeling of pressure |
Moderate | The bladder presses into the vagina and creates a feeling of heaviness or discomfort | Pelvic heaviness, urinary incontinence during activity, frequent urge to urinate |
Severe | Part or all of the bladder protrudes from the vaginal opening (complete prolapse) | Severe pain and pressure, difficulty urinating or passing stool, and problems with sexual intercourse |
When is bladder prolapse surgery necessary?
Bladder prolapse (cystocele) does not always require surgery. In early and mild stages, many people can control symptoms well by strengthening the pelvic floor muscles (Kegel exercises), managing weight, or using methods such as laser therapy to improve tissue quality.
The key point in deciding on bladder prolapse surgery is when the main supporting structures of the pelvis have been damaged enough that nonsurgical methods are no longer efficient and effective. Below, we describe situations in which cystocele surgery is likely to be needed:
Severity of prolapse: when the grade of bladder prolapse is moderate to severe and the bladder reaches the vaginal opening or even protrudes beyond it.
Ineffectiveness of nonsurgical methods: if a person has regularly performed pelvic-floor exercises for months or used a pessary to keep the bladder up, but symptoms remain bothersome or are worsening.
Reduced quality of life: if bladder prolapse symptoms seriously interfere with daily activities, sexual relations, exercise, or work
Difficulty urinating: severe bladder prolapse can bend the urethra and cause incomplete bladder emptying. As a result, a person may need to press on the vaginal wall to urinate.
Urinary incontinence: leakage of urine while coughing, laughing, or sneezing is another sign that, if present, should prompt evaluation for medication therapy and then surgery.

How is laparoscopic bladder prolapse surgery performed?
In this minimally invasive operation, the doctor returns the bladder to its normal position without the need for large incisions. Laparoscopic bladder prolapse surgery is a very suitable option for patients seeking a shorter recovery period and less pain. Below, we explain how this operation is performed:
Steps and technique of laparoscopic bladder prolapse surgery
This operation is performed under general anesthesia or spinal anesthesia and usually takes 1 to 2 hours. The patient is usually hospitalized for 24 hours after surgery and can then walk and perform light activities. The general steps are described below:
1. Preparation and anesthesia: the patient receives general or spinal anesthesia so that no pain is felt.
2. Creating small incisions: the surgeon makes 2 to 4 very small incisions (about half to 1 centimeter) in the lower abdomen near the bikini line.
3. CO2 gas insufflation: harmless carbon dioxide gas is injected into the abdomen through one of the incisions to create enough space for instrument movement and better visualization for the surgeon.
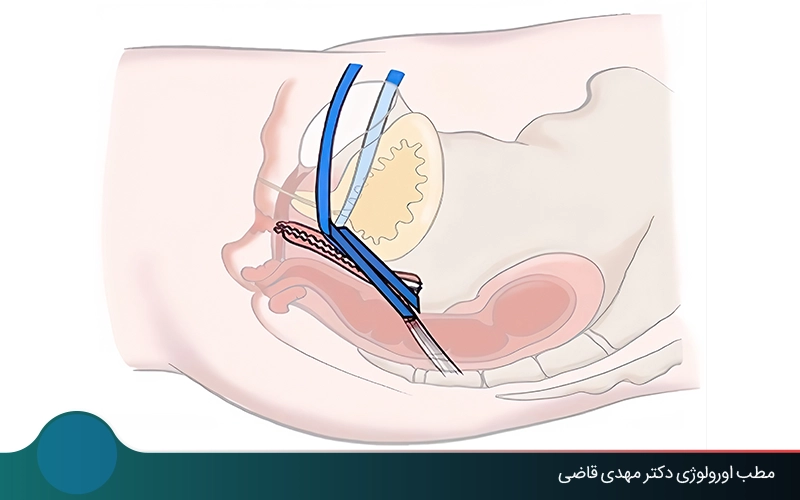
4. Inserting the laparoscope: a small, narrow telescope (laparoscope) equipped with a camera and light is inserted through one of the incisions so images from inside the body are transmitted to a monitor.
5. Lifting and fixing the bladder: using very fine laparoscopic instruments, the surgeon lifts the prolapsed bladder upward. Then, using mesh or strong sutures, it is attached and fixed to bone or stronger pelvic ligaments. This provides lasting support for the bladder.
6. Completing the operation: after the bladder is stabilized, the instruments are removed and the CO2 gas is evacuated. Finally, the small incisions are closed with sutures.
Differences between laparoscopy and open or vaginal surgery
The difference between laparoscopic, open, and vaginal surgery lies in the main approach and clinical outcomes. The table below briefly and usefully summarizes the features of these three surgical models:
Feature | Laparoscopic surgery | Vaginal surgery | Open abdominal surgery |
|---|---|---|---|
Access route | Through small abdominal incisions | Through the vagina (without an external incision) | Through a large abdominal incision |
Degree of invasiveness | Very minimally invasive | Minimally invasive | Invasive |
Repair strength | Excellent and durable (strong mesh can be used) | Good (native-tissue repair, higher chance of recurrence) | Excellent (direct and strong repair with mesh) |
Postoperative pain | Low | Moderate | High |
Recovery period | Short (1 to 2 weeks) | Moderate (2 to 4 weeks) | Long (4 to 6 weeks) |
Hospital stay | 1 to 2 nights | 1 night | 2 to 5 nights |
Scar | 1 to 5 very small scars | No external scar | One large and visible scar |
Use | Preferred and modern method | Common for mild cases and when mesh is not desired | Used less often |
Advantages and disadvantages of laparoscopic bladder surgery
In recent years, laparoscopic bladder surgery has been recognized as one of the most effective and safest methods for repairing bladder prolapse. Of course, like any other surgery, this method has its own advantages and limitations, which we review below:
Key advantages of laparoscopic bladder surgery
Choosing laparoscopy to treat cystocele offers several benefits for the patient and affects the speed of recovery and quality of life after surgery. Below, we discuss these advantages:
Small incisions and minimal scars on the abdominal skin;
Less pain and reduced need for strong painkillers after surgery;
Shorter recovery period and faster return to daily activities;
Lower chance of infection or internal adhesions compared with open surgery;
Better scar appearance than open surgery, especially for younger patients;
Greater surgical precision in fixing the bladder and repairing tissues with the help of magnified imaging.
Possible complications and limitations of laparoscopic bladder prolapse surgery
Although this method is low risk, laparoscopic cystocele surgery may rarely be associated with complications. It is important to know that the rate of these complications in specialized centers is very low:
Table of possible complications of laparoscopic bladder prolapse surgery | |
|---|---|
Possible complication | Details |
Urinary tract infection | Caused by temporary use of a urinary catheter or incomplete bladder emptying in the first days after surgery |
Temporary pelvic and shoulder pain | Due to the use of carbon dioxide gas to create the operative space; usually mild and resolves within a short time. |
Bleeding or clot formation | It can occur, but is usually preventable with anticoagulant medications. |
Possible injury to the bladder, bowel, or ureter | A very rare complication, especially when the operation is performed by experienced surgeons. |
Possibility of recurrent prolapse or need for repeat surgery
One of the main concerns for patients is the possibility of prolapse returning after surgery. Success rates in prolapse surgeries performed with laparoscopic technique and strong fixation, often with mesh, are very high. In a small percentage of patients, a mild form of prolapse may recur, which usually does not require surgery and is controlled with care.
According to an article in Journal of Clinical Medicine, only in limited cases (between 4.8 and 5.7 percent of patients based on body mass index) may secondary repair surgery be needed. The possibility of recurrent bladder prolapse depends on the severity of the initial prolapse, the patient’s general health, and adherence to postoperative care.
Care and recovery points after bladder prolapse surgery

Recovery and postoperative care play an important role in the long-term success of surgery and prevention of recurrent prolapse. Below are several points for initial care and a better recovery period:
Discharge and return to daily activities: you will probably be discharged 24 to 48 hours after surgery and can return to light daily activities within 1 to 2 weeks.
Avoiding pressure on the pelvis: in the first days after surgery, avoid prolonged sitting or standing. For at least 6 to 8 weeks, avoid lifting objects heavier than 3 to 5 kilograms.
Incision care: laparoscopic incisions should be kept clean and dry, and you should follow your doctor’s instructions for dressing changes and bathing.
Preventing constipation: to reduce pressure on the pelvis, follow a fiber-rich diet and drink enough water. If needed, use laxatives prescribed by your doctor.
Sexual intercourse: avoid sexual intercourse until the internal wounds have completely healed. The doctor usually determines restarting after about 6 weeks.
Pelvic-floor exercises: after your doctor approves, start Kegel exercises to strengthen your pelvic-floor muscles and provide long-term support for the bladder.
Factors affecting the cost of laparoscopic bladder prolapse surgery

The cost of laparoscopic bladder prolapse surgery depends on several factors, and a fixed amount cannot be considered for all patients. Technical details of the operation and the patient’s individual condition have a major effect on the final cost. Below, we describe the most important factors affecting the cost of this surgery:
Grade of bladder prolapse: the greater the severity of prolapse and the greater the need for tissue repair, the more the operation time and cost increase.
Type of anesthesia: general anesthesia usually costs more than spinal anesthesia or local methods.
Hospital or surgical center: fees differ among private, semi-private, and public centers.
History of childbirth or previous pelvic surgeries: in patients who have had several deliveries or pelvic operations, surgery will be more complex and time-consuming.
Need for mesh (repair net): in some cases, a special mesh is used to strengthen the bladder wall and has a separate cost.
Summary
Laparoscopic bladder prolapse surgery is a modern, safe, and effective method for treating cystocele. It is associated with small incisions, less pain, and a shorter recovery period. With the skill of experienced surgeons, this method usually has very satisfactory results and patients can return to daily life within a short time. The complication rate in laparoscopic surgery is low, and the chance of recurrent bladder prolapse is also very small.
If you have symptoms of bladder prolapse or plan to undergo this operation, you can see a urology specialist for expert consultation. The urologist will perform the necessary evaluations and prescribe the best treatment method for you.
Frequently asked questions
Actions & related links
Related articles
All articlesWhat Is Polycystic Kidney Disease? (Fetal and Adult PKD)
What is polycystic kidney disease? Learn about inherited ADPKD and ARPKD, fetal and adult symptoms, complications, diagnosis, medicines, surgery, diet, fluids, and prevention-focused care.
What Is a Renal Cortical Cyst? Symptoms, Diagnosis, and Treatment
Renal cortical cyst | Simple vs. complex kidney cysts | Warning symptoms | Diagnosis and treatment | Needle drainage, laparoscopy, medication, and ablation
Kidney Transplant: Cost, Blood Type Compatibility, and Surgical Method
What is kidney transplant? Learn about cost considerations, operation duration and method, diet, who may not be eligible, success rates, isolation precautions, and post-transplant care.
What Is Pyelonephritis? Kidney Infection Symptoms, Diagnosis, and Treatment
What is pyelonephritis? Learn kidney infection symptoms in women, children, men, and pregnancy; diagnosis, antibiotics, treatment, emergency warning signs, and cystitis differences.
Comments
0 comments
No comments yet. Be the first to share your thoughts.