
 Tap to zoom
Tap to zoomBenign Urethral Lesions in Adults
Benign urethral lesions such as strictures, warts, polyps, cysts, caruncles, and prolapse can cause pain, bleeding, or weak urine flow. Learn causes, diagnosis, and treatment options.
- Published on
- June 25, 2026
- Reading time
- 5 min read
- Last updated
- Updated: June 27, 2026
The urethra is a vital part of the urinary system and plays an important role in draining urine from the body. In men, it also has other important functions, including carrying semen. Sometimes, for several reasons, it can develop benign (non-cancerous) lesions.
These lesions may cause symptoms such as narrowing, pain, bleeding, or difficulty emptying the bladder, and they can affect a person's day-to-day life.
In this article, we explain the common causes of benign urethral lesions, the different types of these problems, warning symptoms, and advanced diagnostic and treatment methods.
If you or someone close to you is dealing with problems such as urethral stricture, urethral warts, polyps, or other non-cancerous lesions, this article can help you understand these conditions better and choose the most appropriate treatment approach.
How does the urethra normally work?
The urethra is a vital part of the urinary system. Its main function is to drain urine from the bladder to the outside of the body. This narrow, flexible tube helps remove liquid waste from the body, and its structure differs significantly between men and women:
The male urethra:
The urethra starts at the bladder and passes through the prostate gland. It then travels through the perineum (the area between the scrotum and the anus) and finally along the length of the penis before opening outside the body. In addition to carrying urine, it has a dual role and also serves as the passage for semen during ejaculation.The female urethra:
The female urethra is much shorter than the male urethra. It begins at the bladder, passes through the anterior wall of the vagina, and ends at a small opening near the vaginal entrance. Because the female urethra is shorter, women are more prone to some urinary tract infections.
Under normal conditions, this passage works freely and without obstruction, allowing urine to pass easily and without pain. Any change or blockage in urethral function can cause problems such as weak urine flow, pain, or infection.
What causes urethral lesions?
Urethral lesions are conditions in which the structure or function of the urethra is damaged or disrupted for different reasons. These lesions may be mild or serious and can produce a range of symptoms and complications depending on the cause. Some of the most common causes of urethral lesions include:
Urethral abscess:
A collection of infection and abscess formation in the tissues around the urethra can damage or block this passage. This condition is usually associated with symptoms such as pain, swelling, and difficulty urinating.Pelvic fracture:
Severe injuries and fractures of the pelvic bones may put pressure on the urethra or tear it. These injuries often require surgical intervention.Trauma to the perineum:
A direct blow or severe pressure to the perineum (the area between the anus and the genitals) can injure the urethra and cause problems such as bleeding, pain, and urinary obstruction.Infections:
Urinary tract infections or local infections around the urethra can cause inflammation and tissue damage in this area. Chronic infections increase the risk of scarring and narrowing of the urethra.Injury from medical instruments:
Use of medical instruments such as a urinary catheter or cystoscope can sometimes injure urethral tissues, especially if the procedure is not performed carefully.Congenital conditions:
Anatomical abnormalities present from birth, such as urethral stenosis or fistulas, can disrupt normal urethral function and lead to different complications during life.
Identifying the exact cause of a urethral lesion is very important for effective treatment, and consultation with a urologist may be needed.
Non-cancerous urethral lesions are a group of benign but sometimes troublesome conditions that can disrupt normal urine flow and cause a variety of symptoms.
Each of these problems has specific features. Recognizing them requires medical precision and diagnostic tools such as cystoscopy or advanced imaging. Below, we review these lesions, common symptoms, and related treatment methods in more detail.
Urethral warts: a common but preventable lesion
Urethral warts are benign but potentially problematic lesions of the urinary tract. In men, they are usually associated with warts on the shaft of the penis. These lesions most often develop because of infection with human papillomavirus (HPV). HPV is one of the most common sexually transmitted infections. It is transmitted through sexual contact and can cause lesions inside the urethra as well as genital warts.
Warts inside the urethra may cause no symptoms, or they may present with changes in urine stream, blood at the start of urination, or discomfort during urination. Lesions seen by a doctor at the urethral opening are a warning sign that more detailed evaluation is needed. Cystoscopy or HPV-related testing may be needed for a definite diagnosis.
If urethral warts are not treated, they can lead to partial or complete urethral obstruction, secondary infections, or spread of the virus to other parts of the genital tract. Some HPV strains, although less commonly, are associated with a higher risk of cancers of the genital and anal regions.
Urethral warts can largely be prevented with HPV vaccination and safer-sex practices. People with infection should also remain under regular medical follow-up to help prevent spread of infection and possible complications.
Treatment of genital warts inside the urethra
genital warts inside the urethra, caused by human papillomavirus (HPV), are among the more challenging HPV-related lesions. These warts usually appear near the urethral opening or inside the urethra and can cause symptoms such as burning, obstruction of urine flow, or bleeding.
Treatment requires careful assessment and selection of appropriate treatment methods to reduce symptoms and control the lesions.
Treatment methods for warts inside the urethra:
Laser ablation:
CO₂ or Nd:YAG laser is commonly used as one of the main methods for treating warts inside the urethra. Laser treatment helps remove lesions with high precision while minimizing damage to surrounding healthy tissue. It is especially useful for larger warts or warts resistant to other treatments.Cryotherapy:
Freezing with liquid nitrogen or other cryotherapy agents can remove small urethral warts. However, this method is limited by the difficulty of reaching deeper warts inside the urethra.Endoscopic resection:
When warts cause obstruction or severe symptoms, endoscopic methods may be used to remove them. In this approach, the warts are removed under direct vision using a cystoscope and fine surgical instruments.Topical medications:
Topical treatments such as podophyllin are usually prescribed for external warts, but their use inside the urethra is limited. Because this area is sensitive, these medicines must be used cautiously and under medical supervision.Electrocautery:
This method uses electric current to destroy wart tissue. Electrocautery is usually performed under anesthesia and is used particularly for lesions that are resistant to other treatments.
The risk of wart recurrence after treatment is high, and periodic follow-up is needed.
None of these methods guarantees complete eradication of the virus, because HPV may remain latent in the tissue.
Lichen sclerosus (LS) or balanitis xerotica obliterans (BXO)

Lichen sclerosus or balanitis xerotica obliterans is a chronic skin disease that usually appears in the penile area. It particularly affects the glans penis and the skin around the urethral opening (urethral meatus). Although its exact cause is still unknown, autoimmune factors, genetics, and chronic inflammation are thought to contribute to the disease.
The disease may begin with pale, shiny, white skin around the urethral meatus. Over time, this tissue may become firm, adherent, and turn into white scar tissue. Lichen sclerosus often begins in childhood and, if untreated, may progress into adulthood.
Symptoms of lichen sclerosus
Urethral stricture: One common problem in this disease is gradual narrowing of the urethra, which can make urination difficult.
Pain and discomfort: Patients may have pain, itching, and a burning sensation in the affected area.
Skin fissures and sores: The disease may cause cracking of the skin, ulceration, and sometimes bleeding.
Difficulty retracting the foreskin: Uncircumcised men with lichen sclerosus often have difficulty pulling back the foreskin.
Complications of lichen sclerosus
If untreated, this disease can lead to more serious complications, including:
Genital cancer: Although rare, chronic lichen sclerosus can increase the risk of squamous cell carcinoma.
Urethral obstruction: Severe narrowing may require urologic surgery.
Recurrent infections: Fissures and sores increase the risk of infection.
Sexual problems: In some cases, problems with sexual function may occur.
Treatment of lichen sclerosus (LS) or balanitis xerotica obliterans (BXO)
Treatment of lichen sclerosus (LS) or balanitis xerotica obliterans (BXO) focuses on reducing inflammation, preventing progression of scarring, and managing complications such as urethral stricture. First-line treatment includes potent topical corticosteroids such as clobetasol propionate, prescribed to control inflammation and prevent disease progression. If the patient does not respond adequately, calcineurin inhibitors such as tacrolimus or pimecrolimus may be recommended.
In patients with severe urethral narrowing or phimosis who have not responded to medication, circumcision may be performed as an effective surgical treatment. If LS has caused urethral stricture, urethroplasty, which reconstructs the narrowed segment using buccal mucosa graft or other healthy tissue, may be performed. In early stages of urethral narrowing, dilation may be used temporarily, but it is not considered a definitive treatment.
In selected cases, CO₂ laser may be used to modify scar tissue or reduce the severity of narrowing. Some studies have also discussed platelet-rich plasma (PRP) to improve tissue quality and reduce inflammation, but this method still needs stronger scientific evidence.
If secondary infections occur, appropriate antibiotics or antifungal medicines are prescribed. Treatment should be tailored to symptom severity and the patient's condition, and patients need periodic follow-up to prevent recurrence and assess treatment results.
Urethral stricture
Urethral stricture occurs when parts of the urethra become narrowed because of injury or chronic inflammation instead of remaining normally open. The main cause of this narrowing is scar tissue, a firm abnormal layer that forms as the body's response to injury or ongoing irritation.
Imagine the smooth, flexible wall of the urethra gradually being replaced by internal scarring; instead of complete healing, the scar creates a stiff, adherent structure. This change can be like closing a main road: it disrupts smooth urine flow and forces it through a narrow passage. In some cases, the obstruction becomes so severe that urine flow almost stops completely.
This gradual but damaging process may be caused by physical trauma, recurrent infections, or even medical procedures that put pressure on the urethra. For this reason, recognizing these changes and diagnosing them early is very important.
Symptoms of urethral stricture include:
Persistent weak urine stream
Frequent urination
Urinary tract infections
Bleeding
A urologist identifies urethral stricture using urinalysis, X-ray imaging (retrograde urethrography), and looking inside the urethra with a long, thin camera with a light at its tip (cystoscope).
Treatment of urethral stricture
To treat urethral stricture, the urologist must know where the narrowing is located. This is done with an X-ray study called urethrography.
A special contrast dye is injected into the urethra through the tip of the penis.
During the X-ray, this contrast material shows the location and length of the stricture.
If strictures are very long and severe, or if they completely block the urinary channel, the urethra may be so narrow that a catheter cannot pass through it. In that situation, a small procedure may be needed to temporarily place a catheter through the lower abdomen below the navel into the bladder so urine can drain from that site (suprapubic catheter or cystostomy).
Urethral stricture is often treated in one of two ways: dilation (widening) or surgery.
Dilation or widening of the urethra
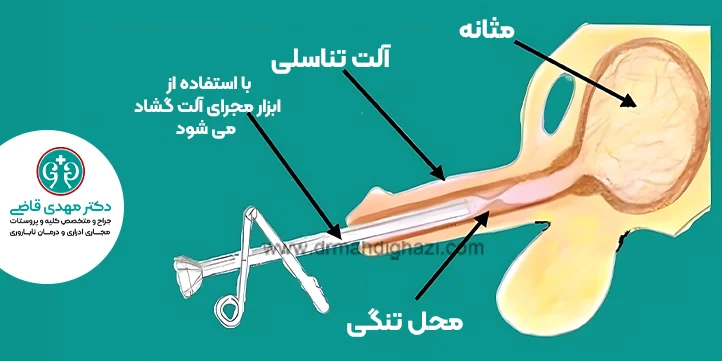
Dilation is a method used to open a narrowed urethra and return it to its normal width.
A catheter is passed through the tip of the penis into the bladder.
Each time, the catheter is removed and a slightly larger catheter is used until the opening reaches the appropriate width. This procedure is performed with anesthetic gel inside the urethra.
The urologist uses a cystoscope (a urologic endoscope) to examine the urethra. Dilation under local anesthesia can cause discomfort, and it is more painful for tougher and longer strictures.
The urologist may leave a special catheter in the urethra for 24 hours or longer to drain the bladder.
Dilation is often useful for short strictures.
If dilation has already been used to treat the stricture, the stricture may recur.
The timing of recurrence varies, so this treatment may be temporarily useful for some patients.
Internal urethrotomy (direct vision internal urethrotomy)
Direct vision internal urethrotomy, abbreviated DVIU, is one effective method for treating short urethral strictures less than 2 centimeters long. In this procedure, the urologist uses a cystoscope to enter the urethra. A small knife or laser is then guided into the urethra and a precise, deep incision is made at the narrowed segment. This incision opens the urethra and improves urine flow.
Internal urethrotomy is usually performed under general anesthesia or spinal anesthesia, and after surgery the patient will need temporary urinary catheterization to keep the urethra open. Recovery is short, and patients can often return to daily activities after a few days.
Although internal urethrotomy gives good results in selected cases, stricture recurrence is possible. In that situation, repeat surgery or alternative methods such as urethroplasty may be needed. The decision depends on the severity and location of the stricture, the patient's condition, and the physician's experience.
Urethroplasty

Long strictures and scars in the penile urethra do not respond well to internal urethrotomy or dilation.
These scars, and a urethra that has been completely obliterated, can be repaired by reconstructive urethral surgery (urethroplasty).
Urethroplasty is performed through open surgery. The penis or perineum is opened with a surgical incision, and the scarred segment of the urethra is removed.
After the narrowed segment is removed, the two healthy ends of the urethra are joined again with fine sutures.
Sometimes the stricture is very long, and if the diseased urethra is removed, there is not enough remaining urethra to connect the two healthy ends.
In that case, to avoid shortening the final length of the urethra, a graft or skin substitute is used to replace the urethra at the narrowed area, and a segment of urethra is reconstructed with the graft so the real urethral length is preserved. This tissue may be taken from the inside of the cheek or another part of the body.
After this surgery, a catheter is needed for several weeks.
Permanent metallic stents are sometimes used to relieve urethral stricture in the prostatic urethra and proximal penile urethra, but these stents are not useful for most patients.
Urethral polyp
Urethral polyps are small, benign tissue growths that are usually present from birth. They are seen more often in women and may appear at the urethral opening or near the vaginal opening.
Polyps are often made of firm, dense tissue, but other components may also be present in their structure, such as smooth muscle, small cysts, or fine nerve tissue, all covered by a thin protective layer. This tissue composition means polyps may sometimes feel like soft masses and sometimes like firm protrusions.
Common symptoms of a urethral polyp
A lump at the vaginal opening or urethral meatus: A mass that may be visible by touch or inspection.
Blood in the urine (hematuria): Polyps may sometimes bleed, and the blood can be seen in the urine.
Obstruction of urine flow: In some cases, a polyp can partially block the urethra and make emptying the bladder difficult.
How is a polyp diagnosed?
To diagnose urethral polyps, the urologist uses the following methods:
Cystoscopy: A thin instrument with a camera used to directly view the inside of the urethra and the polyps.
X-ray imaging: Techniques such as voiding cystourethrogram (VCUG) or retrograde urethrography (RUG) are used to define the structure and exact location of the polyps.
These evaluations not only help diagnose a polyp but also allow assessment of its effect on normal urinary tract function.
Treatment of a urethral polyp
A urethral polyp is a rare benign lesion that is usually related to chronic irritation, inflammation, or congenital factors. Treatment depends on the size, location, and symptoms, and the goal is complete removal of the lesion and relief of symptoms.
The standard treatment for a urethral polyp is surgery. Polyps are usually removed under direct vision with endoscopic techniques such as cystoscopy. This method is minimally invasive and has a short recovery time. If the polyp is large or causes significant bleeding, open surgery may be needed to remove it.
If there is evidence of infection associated with the polyp, an appropriate antibiotic is prescribed before surgery. After removal, the specimen is sent for pathologic examination to rule out any possibility of malignant change.
In patients with recurrent polyps, underlying causes such as chronic irritation or urinary stones should be evaluated. Treating these factors can help prevent recurrence. Periodic follow-up is also important to assess the patient's condition and prevent the lesion from returning.
Paraurethral cyst
Paraurethral cysts also known as Skene's gland cysts are benign masses that form in the anterior vaginal wall near the female urethra. These glands have a small role in lubricating the urethra, but if their ducts become blocked, fluid can accumulate and appear as a cyst.
These cysts are usually seen as firm, shiny, raised masses that are white to yellowish in color. If the cyst enlarges, it can narrow the urethra and disrupt normal urine flow.
Common symptoms of a paraurethral cyst
Palpable mass: Usually felt in the anterior vaginal wall and may cause discomfort.
Deflected urine stream: The cyst can change the direction of urine flow and cause abnormal emptying.
Urinary obstruction: In severe cases, the cyst may make urine outflow difficult.
Painful urination (dysuria): Pressure from the cyst on the urethra can cause pain during bladder emptying.
These cysts are usually identified on physical examination because of their typical location and appearance. They may be associated with discomfort or obstructive symptoms, but they are often benign and require more detailed evaluation or treatment only if they cause more serious symptoms.
A definite diagnosis is usually made with imaging studies and clinical assessment by a urologist.
Treatment of a paraurethral cyst
A paraurethral cyst, which usually develops near the urethra and in the tissues around it, may form because of obstruction of the paraurethral glands or infection. In some cases these cysts cause no symptoms and do not need treatment, but treatment is needed if they cause pain, urinary obstruction, infection, or discomfort.
The main treatments for a paraurethral cyst include:
Drainage:
If the cyst is infected or large, its contents are drained using simple surgical techniques or endoscopic guidance. This method is effective for rapid symptom relief and for preventing further infection.Marsupialization:
If the cyst recurs repeatedly or is large, marsupialization surgery is performed. In this method, the cyst is opened and its edges are sutured to the skin to create a tract for natural drainage and prevent the cyst from closing again.Complete cyst excision:
If the cyst recurs repeatedly or is suspicious for pathologic change, complete surgical excision is performed, with full separation of the cyst from the surrounding tissues.Antibiotics:
If the cyst is associated with infection, appropriate antibiotics are prescribed before or after drainage to prevent spread of infection.Follow-up:
After treatment, periodic follow-up is necessary to assess treatment success and prevent recurrence. If new symptoms occur or the cyst returns, re-evaluation and appropriate management are important.
Treatment should be selected according to symptom severity and the patient's condition. Sending the cyst specimen for pathologic examination after removal is important, especially in suspicious cases, to rule out malignancy.
Urethral caruncle
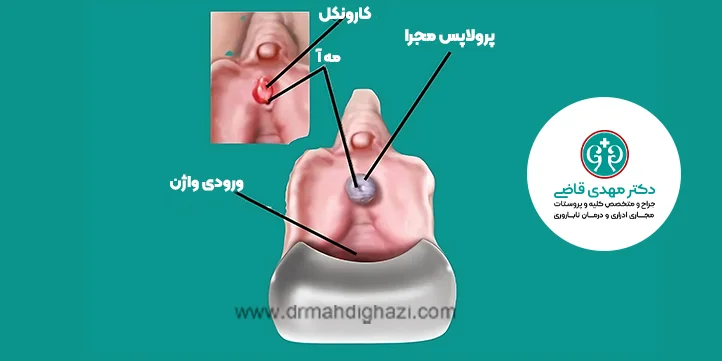
Urethral caruncle is a type of polypoid (stalked) mass that protrudes from the urethral opening or urethral meatus. These small, red lesions are usually seen during routine examinations or during evaluation of other problems.
Caruncles are more common in women who are postmenopausal and are not using hormone replacement therapy (HRT). This is related to lower estrogen levels and hormonal changes, which make genital and urethral tissues thinner and more sensitive.
A caruncle usually appears as a small red mass with a thin membrane protruding from the urethral opening. Because of its location and the sensitivity of the tissue, it may cause pain or discomfort when touched or during urination.
Common symptoms of a urethral caruncle
Pain and bleeding during urination: Irritation or injury to the lesion can cause discomfort or bleeding.
Frequent urination: The need to urinate repeatedly, even in small amounts.
Sudden need to urinate (urgency): A strong feeling that the bladder must be emptied immediately.
Tenderness at the urethral opening: The urethral meatus may be tender or inflamed.
Caruncles are mostly related to menopausal changes and reduced estrogen hormone levels. This hormonal decline can cause tissue atrophy, thinning of the skin, and increased susceptibility to formation of these masses.
These lesions are usually benign and rarely cause a serious problem, but if significant symptoms or discomfort occur, more detailed evaluation by a urologist is necessary.
Treatment of a urethral caruncle
A urethral caruncle is a benign inflammatory lesion that usually develops in postmenopausal women at the urethral opening. It may be asymptomatic, but in some cases it causes symptoms such as pain, bleeding, or burning with urination. Treatment depends on lesion size, symptom severity, and response to initial therapy.
Medical treatments:
When the caruncle is small and causes mild symptoms, conservative treatment is preferred. This treatment includes:Topical estrogen: Use of estrogen creams to reduce inflammation and improve tissue quality in postmenopausal women.
Anti-inflammatory ointments: Such as hydrocortisone, to reduce swelling and inflammation.
Surgical treatment:
If the caruncle is large, does not respond to conservative treatment, or causes recurrent and severe bleeding, surgical removal is recommended. This procedure is usually performed as an outpatient procedure under local anesthesia. The removed lesion is sent for pathologic examination to rule out malignant change.Treatment of secondary infections:
If the caruncle is associated with infection, an appropriate antibiotic is prescribed.Follow-up:
After treatment, regular follow-up is necessary to monitor the patient's condition and ensure the lesion has not recurred.
In most cases, conservative treatment or surgery leads to complete improvement, but follow-up is recommended to confirm successful treatment and complete resolution of symptoms.
Urethral prolapse
Urethral prolapse is a rare condition in which the inner lining of the urethra and the tissue beneath it protrude outward from the urethral opening (urethral meatus). This condition causes pain, bleeding, and sometimes obstruction of urine flow. Unlike many benign lesions, urethral prolapse usually causes more discomfort for the patient.
Who is at risk of urethral prolapse?
This problem is seen more often in young girls, but it can occur at any age. Several factors, such as weakness of local tissues, repeated pressure on the urethra (for example, chronic cough or severe constipation), or hormonal changes, can contribute to the condition.
Common symptoms of urethral prolapse:
Protrusion of the inner urethral lining and the underlying spongy tissue
Swollen, red, and tender appearance
Severe pain in the genital area
Bleeding from the vagina or around the urethral meatus
Difficulty emptying urine or urinary obstruction
Feeling of pressure or heaviness in the genital area
Urethral prolapse is usually identified by clinical examination of the genital area. By carefully examining the area, the urologist can distinguish this condition from similar problems such as polyps or urethral masses.
Urethral prolapse is usually easy to recognize because of its typical appearance and prominent symptoms, but specialist evaluation is needed to assess severity and choose the appropriate treatment method.
Treatment of urethral prolapse
Urethral prolapse, seen most often in prepubertal children or postmenopausal women, refers to protrusion of the urethra from its opening. It can cause symptoms such as bleeding, a feeling of a mass in the genital area, and discomfort during urination. Treatment depends on symptom severity and the patient's condition and may include conservative or surgical methods.
Non-surgical treatments:
These methods are used when prolapse is mild or does not cause severe symptoms:Topical estrogen:
Use of estrogen creams helps strengthen local tissues and reduce prolapse, especially in postmenopausal women.Anti-inflammatory ointments:
Used to reduce inflammation and swelling.Warm sitz baths:
Help reduce pain and discomfort by soothing injured tissues.
Surgical treatment:
If conservative treatments are not effective, or if prolapse causes severe bleeding, infection, or urinary obstruction, surgery is recommended. Surgical methods include:Resection of the prolapse and urethral repair:
Removal of the protruding tissue and reconstruction of the area to return the urethra to its normal position.Urethral fixation:
In some cases, the urethra is fixed to surrounding walls to prevent recurrence of prolapse.
Management of associated complications:
If a urinary tract infection caused by prolapse is present, an antibiotic is prescribed.
Control of bleeding with local compression or surgical methods in severe cases.
Follow-up:
After treatment, patients need regular follow-up to assess treatment success and prevent recurrence of prolapse.
In most cases, urethral prolapse can be controlled with appropriate treatment. The treatment method is chosen according to symptom severity, the patient's age, and overall health status.
Urethral abscesses, injuries, and infections require prompt treatment. Abscesses caused by gonococcal urethritis are treated with antibiotics, and in some cases surgical drainage is needed. A Foley catheter, or in severe urethral narrowing a suprapubic catheter, may be used for urine drainage until full recovery. After recovery, the patient should be able to urinate normally.
Post-treatment care for urethral lesions
Benign lesions related to HPV and gonorrhea are not easily eliminated from the body.
Antibiotics can keep them under control. These urethral lesions often recur and require repeat treatment.
After dilation and internal urethrotomy, the chance of stricture recurrence is high.
This depends on the length of the stricture.
Shorter strictures usually respond better than longer ones.
Many studies show that intermittent urethral catheterization, weekly for up to 3 months after treatment, can help prevent stricture recurrence.
Complications of urethroplasty include:
Stricture recurrence
Bleeding
Infection
Blood clots in the veins of the lower limbs due to long surgery time (this is rare)
Before removing the catheter after surgery, the urologist will probably order a voiding cystourethrogram
(VCUG). This X-ray study shows whether healing is complete.
After surgery for urethral stricture, the urinary tract surgeon often follows the patient at later visits with examination and questions.
The urologist may also order tests to assess the speed and strength of urine flow. Repeat imaging (retrograde urethrogram) is often performed 3 and 12 months after urethroplasty to see whether the stricture has recurred.
Although most strictures recur within one year after surgery, in some cases this period may extend up to 10 years.
Summary
The urethra is a vital part of the urinary system. This delicate and complex structure can sometimes develop benign, non-cancerous lesions for different reasons. Although these lesions are not usually dangerous, they can affect a person's quality of life. They may include urethral warts, urethral stricture, polyps, paraurethral cysts, or specific conditions such as lichen sclerosus.
Urethral lesions may occur because of chronic infections, physical trauma, use of medical instruments such as catheters, congenital factors, or hormonal changes. Their symptoms include pain, bleeding, weak urine flow, or masses in the urethral area, which can sometimes disrupt daily life.
Diagnosis requires specialist evaluation by a urologist and methods such as cystoscopy or advanced imaging. Treatment also varies depending on lesion type and severity, ranging from topical medicines and antibiotics to advanced surgical procedures. For example, urethral warts caused by HPV may be treated with laser therapy or cryotherapy, whereas urethral stricture may require more precise surgery such as urethroplasty.
Post-treatment care, including regular follow-up to prevent recurrence, is very important. Measures such as HPV vaccination and sexual hygiene can also help prevent some of these lesions.
Overall, accurate recognition of these problems and access to appropriate treatment methods help patients reduce symptoms and live healthier, more comfortable lives. This article aims to provide a comprehensive view of the causes, symptoms, and treatment options for benign urethral lesions and to clarify the importance of specialist medical consultation in managing these problems.
Frequently asked questions about benign urethral lesions
Actions & related links
Related articles
All articlesWhat Is Polycystic Kidney Disease? (Fetal and Adult PKD)
What is polycystic kidney disease? Learn about inherited ADPKD and ARPKD, fetal and adult symptoms, complications, diagnosis, medicines, surgery, diet, fluids, and prevention-focused care.
What Is a Renal Cortical Cyst? Symptoms, Diagnosis, and Treatment
Renal cortical cyst | Simple vs. complex kidney cysts | Warning symptoms | Diagnosis and treatment | Needle drainage, laparoscopy, medication, and ablation
Kidney Transplant: Cost, Blood Type Compatibility, and Surgical Method
What is kidney transplant? Learn about cost considerations, operation duration and method, diet, who may not be eligible, success rates, isolation precautions, and post-transplant care.
What Is Pyelonephritis? Kidney Infection Symptoms, Diagnosis, and Treatment
What is pyelonephritis? Learn kidney infection symptoms in women, children, men, and pregnancy; diagnosis, antibiotics, treatment, emergency warning signs, and cystitis differences.