
 Tap to zoom
Tap to zoomWhat Is Hemorrhagic Cystitis and How Is It Treated?
What is hemorrhagic cystitis? Learn about bladder inflammation with bleeding, symptoms, causes, diagnosis, treatment, prevention, and when to see a urologist.
- Published on
- June 26, 2026
- Reading time
- 5 min read
- Last updated
- Updated: June 27, 2026
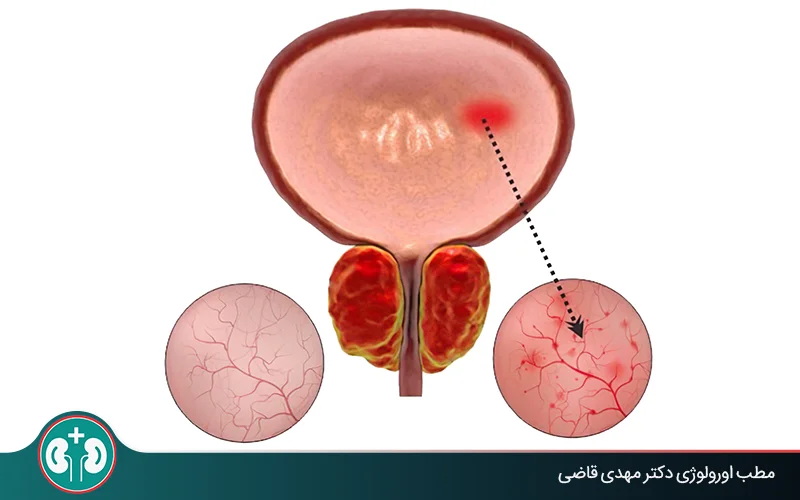
Hemorrhagic cystitis is a type of mild to severe inflammation of the inner lining of the bladder that causes visible blood in the urine (gross hematuria).
This condition can be caused by certain medicines, cancer treatments, and infectious agents, and because bleeding may be severe, it requires urgent evaluation, diagnosis, and treatment.
In this article, we explain the symptoms of hemorrhagic cystitis and then review how it is diagnosed and treated.
Symptoms of Hemorrhagic Cystitis
Symptoms can be mild or severe and dangerous, depending on the extent of bladder injury and the amount of bleeding. In either case, the patient needs medical care.

Visible urinary bleeding (gross hematuria): a change in urine color and possible blood clots;
Symptoms caused by inflammation: burning, frequent urination, and urinary urgency;
Signs of urethral obstruction or urinary retention: feeling that the bladder has not emptied completely, severe pain;
Symptoms related to heavy bleeding: dizziness, severe weakness, or fainting.
How Are the Symptoms of Simple Bladder Inflammation (Cystitis) Different From Hemorrhagic Cystitis?
Hematuria and its severity are the main differences between simple bladder inflammation and hemorrhagic cystitis:
Simple bladder inflammation may cause blood in the urine, but often the amount of blood is so small that it is seen only under a microscope; these cases are called “microscopic hematuria.”
Hemorrhagic cystitis is associated with “gross hematuria,” meaning the urine color changes clearly (pink or bright red to dark brown) and blood clots may also be seen in the urine.
What Causes Hemorrhagic Cystitis of the Bladder?
This condition has several causes, which fall into 2 groups: infectious and noninfectious. In most cases, it is noninfectious and occurs because of chemotherapy and radiation therapy; infectious causes include viruses, bacteria, or fungi. Depending on the cause, the condition may develop after 48 hours, after several weeks, or even after several years.
What are the causes of hemorrhagic cystitis? | |||
|---|---|---|---|
Type of hemorrhagic cystitis | Cause | Speed of symptom onset | Usual time frame |
Noninfectious | Chemotherapy and related medicines | Early onset | 48 hours |
Radiation therapy | Delayed onset | Average of 35 months | |
Bone marrow transplant | Delayed onset | Up to 2 to 3 months after transplant | |
Infectious | BK virus | Delayed onset | Has a latent period | It becomes active in immunocompromised patients and in people who receive transplants and take immunosuppressive medicines. |
Chemotherapy and Related Medicines
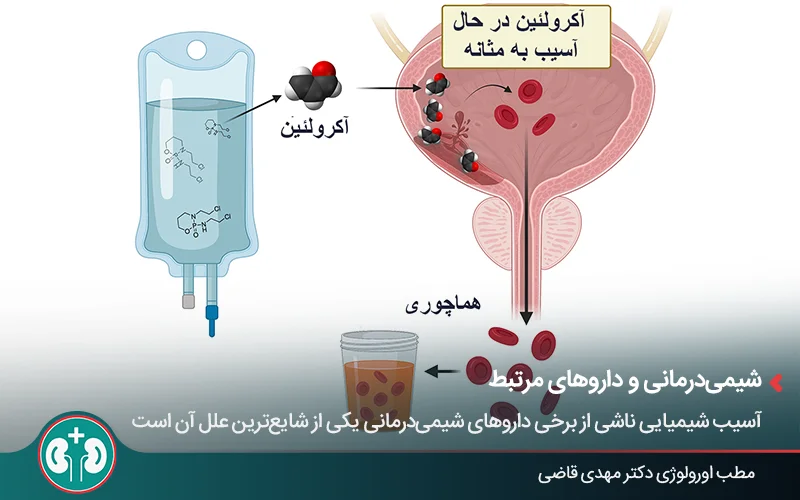
Chemical injury from some chemotherapy medicines is one of the most common causes of hemorrhagic cystitis. In particular, medicines such as cyclophosphamide and ifosfamide are among the main causes of this complication. These medicines may cause bladder bleeding after 48 hours through the following steps:
The medicines are broken down in the liver, and a toxic substance called acrolein is produced.
Acrolein travels through the blood to the urinary tract and eventually reaches the bladder; as a result, the inner lining of the bladder is exposed to this toxic substance.
Acrolein damages cellular DNA and causes cell death (necrosis). The result of this process is inflammation, ulceration, and severe bleeding from the bladder wall.
Radiation Therapy
Radiation therapy is another major cause of hemorrhagic cystitis and can lead to ongoing bleeding from the bladder wall through the following process:
Initial injury: radiation damages the inner lining of the bladder blood vessels;
Reduced blood supply: this injury causes chronic inflammation, gradual blockage of blood vessels and ultimately ischemia (reduced blood flow); as a result, less oxygen reaches the bladder;
Formation of abnormal blood vessels: to compensate for the reduced blood supply, new blood vessels form in the bladder wall that have an abnormal and fragile structure.
Bleeding: these fragile vessels rupture easily and the bladder develops ongoing bleeding.
In an article from the Canadian Journal of Urology (2022), written by researchers from the Department of Urology at Thomas Jefferson University, the authors state: “When radiation therapy is the cause, symptoms often appear after a delay and their timing has been reported at an average of 35 months after treatment.”
Viral and Bacterial Infections
Among infectious causes of hemorrhagic cystitis, viruses are the most common and important cause, especially in patients with a weakened immune system, such as transplant recipients.
BK virus, the main cause, remains latent in the bodies of many people. After the immune system is suppressed, this virus becomes active and multiplies in the lining cells of the bladder (urothelial cells). Its activity can cause complications such as bladder tissue damage and bleeding.
Bacteria and fungi can also cause the condition, but their role is much smaller. Bleeding caused by bacteria and fungal hemorrhagic cystitis are both rare, especially fungal hemorrhagic cystitis, which is usually seen in patients with immune deficiency or in people who have a long-term catheter.
Some other infectious agents:
Adenovirus;
Escherichia coli (E. coli);
Candida fungus.
Bone Marrow Transplant
A “bone marrow transplant” itself is not a direct cause of this condition, but a patient who receives transplanted cells is exposed to other causes of “hemorrhagic cystitis”:
Reactivation of latent viruses (such as BK virus) due to immunosuppressive medicines.
Chemotherapy or radiation therapy.
How Is Hemorrhagic Cystitis Diagnosed?
To diagnose hemorrhagic cystitis accurately, physicians must rule out other possible conditions and identify the main cause of bleeding. This is done through a multistep process that includes “initial patient assessment, blood and urine tests, imaging, and cystoscopy.”
Initial Assessment
The doctor first asks about the patient’s medical history, especially any history of chemotherapy, radiation therapy, or stem cell transplant . A physical examination is also performed to assess pain and overall condition.
In acute situations, the main goal of this assessment is “stabilizing the patient’s circulation,” because severe bleeding can be life-threatening. To do this, the following are checked:
Blood pressure;
Heart rate;
Hemoglobin and hematocrit to assess the amount of blood loss.
Blood Test

In the diagnostic process for hemorrhagic cystitis, blood testing has 2 main goals:
Assessing the severity of bleeding: with a “complete blood count” (CBC), two important measures are checked: the level of hemoglobin (the red blood cell protein) and hematocrit (the percentage of red blood cells in the blood). This test shows whether the patient needs a blood transfusion because of anemia caused by bleeding.
Ruling out blood disorders and other possible causes: by checking platelet counts and coagulation tests such as PT and PTT (tests of clotting speed), the doctor can determine whether factors such as low platelets, hemophilia, or blood-thinning medicines have caused the bleeding.
Types of Urine Tests
Urinalysis shows the severity of hematuria and helps rule out other possibilities such as bleeding from the kidneys. Urine cytology results can also help identify other possible causes, such as bladder cancer.
Imaging
Using imaging methods such as ultrasound and CT urogram, the doctor checks for other possible causes of hematuria, such as urinary stones or bleeding from the kidneys and ureters.
Cystoscopy
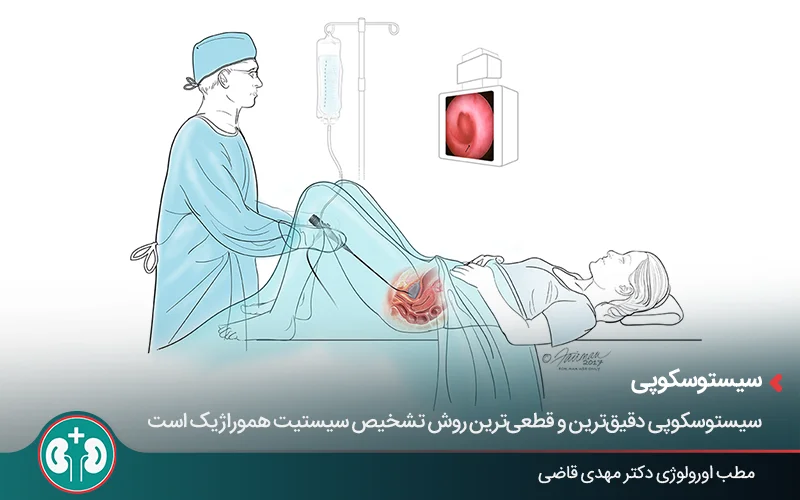
Cystoscopy is the most accurate and definitive method for diagnosing hemorrhagic cystitis and allows the doctor to see inside the bladder, assess the severity of injury, and, if needed, treat bleeding at the same time by cauterizing blood vessels. The list below includes the most important findings checked during cystoscopy:
Inflammation and redness;
Swelling of the mucosa;
Fragile tissue that bleeds with minimal contact;
Active bleeding points;
Abnormal, dilated blood vessels;
Presence of a bladder stone or tumor.
How Is Hemorrhagic Cystitis Managed and Treated?
Successful management of this condition requires a step-by-step approach . This process starts with the least invasive treatments and, if needed, continues with more invasive options.
1. Initial and Supportive Measures
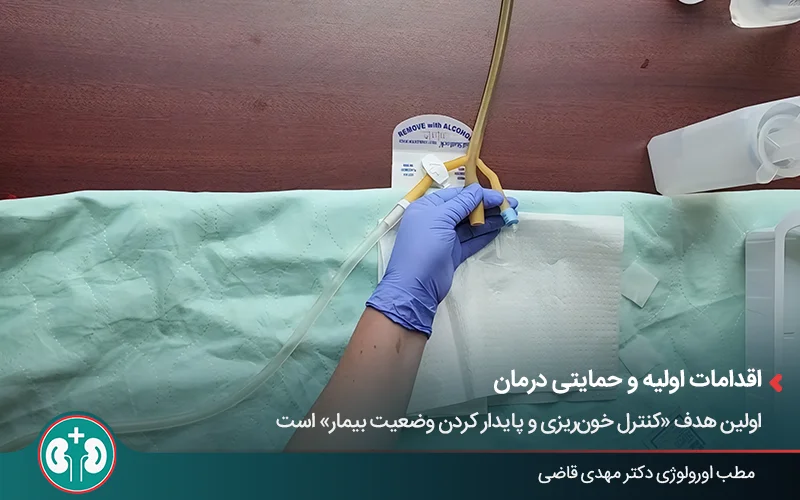
The first goal is “controlling bleeding and stabilizing the patient”; therefore, this stage of treatment includes the following measures:
Supportive care: the first step is stabilizing circulation in the patient. This includes “intravenous fluids, blood transfusion, and correction of any clotting disorder”.
Emptying the bladder and removing clots: to relieve urinary retention or prevent it, the patient’s bladder is drained using a type of catheter.
Continuous bladder irrigation: after drainage, the bladder is continuously irrigated through a three-way catheter so new clots do not form.
2. Surgical Interventions
If initial measures are not effective and bleeding continues, the doctor performs 2 important steps through cystoscopy under anesthesia:
Removal of remaining blood clots;
Cauterization of the bleeding blood vessels.
3. Intravesical Irrigation With a Medicinal Solution
If cystoscopy and cauterization are also not effective, the next step is to instill certain chemicals directly into the bladder to control bleeding chemically.

Alum causes various protein compounds to precipitate at the bleeding site. These protein deposits create a protective layer and stop the bleeding.
Silver nitrate works in a way similar to alum.
Formalin is considered a last resort for controlling very severe bleeding that is resistant to treatment because it has strong caustic effects. This medicine may cause serious complications, such as a permanent decrease in bladder capacity.
4. Repair-Oriented and Adjunctive Methods
Hyperbaric oxygen therapy is a noninvasive, repair-oriented method with the greatest effect in cases caused by radiation therapy. This method is not effective for controlling acute bleeding and is used for chronic bleeding with the goal of “gradual repair of bladder tissue”.
5. Options for Treatment-Resistant Cases
In acute hemorrhagic cystitis, when bleeding does not respond to other treatments, physicians move to more invasive options.
Angioembolization
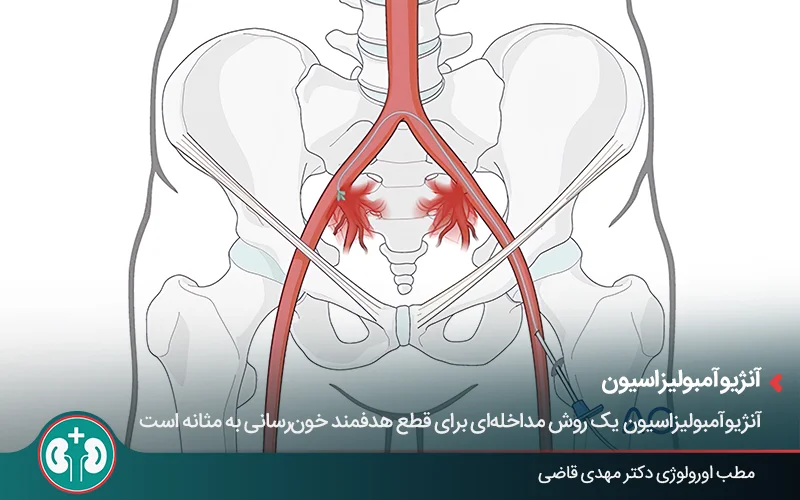
Angioembolization is an interventional procedure for targeted interruption of blood flow to the bladder and is used for severe, localized bleeding from bladder vessels.
To treat this bleeding, an interventional radiologist inserts a thin tube (catheter) into an artery and advances it to the bleeding point; then embolic materials (blocking agents) are injected to block the injured artery and stop the bleeding.
Nephrostomy
This is a temporary measure to protect the kidneys and is used to relieve pressure and prevent kidney injury. When the bladder is full of clots and the patient is unstable, the doctor inserts tubes directly through the skin into the kidneys so urine can drain. This situation continues until the treatments work and the patient becomes more stable.
Cystectomy (bladder removal)
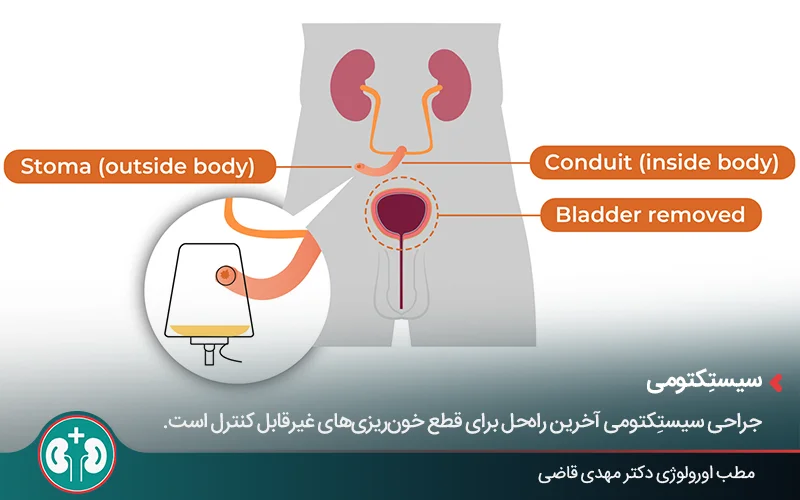
This surgery is the last resort for stopping uncontrollable bleeding. In this operation, the bladder is completely removed to eliminate the main source of bleeding.
Is There a Way to Prevent Hemorrhagic Cystitis?
Prevention of hemorrhagic cystitis depends on its underlying cause. At present, only complications caused by chemotherapy are partly preventable, and there is no definitive preventive method for other main causes such as radiation therapy or viral infections.
Prevention Methods
For patients who are going to receive certain chemotherapy medicines such as cyclophosphamide and ifosfamide, two prevention methods are used at the same time:
12: Mesna ampoule for prevention of hemorrhagic cystitis
1. Mesna: this medicine acts like an antidote to the toxic substance acrolein. It is given intravenously or by mouth just before or at the same time as chemotherapy, and it inactivates acrolein in the urine.
2. Aggressive hydration: in this method, large amounts of fluid, mainly through an intravenous line, are given to the patient so that the concentration of toxic substances in the bladder decreases and they are also flushed from the body faster through frequent urination.
Effectiveness
Mesna has a significant effect, but chemotherapy may still cause hemorrhagic cystitis. According to the source mentioned earlier, when a patient receives the current standard preventive treatment, the risk of developing hemorrhagic cystitis with mesna is usually less than 10%.
When Should You See a Doctor?
In severe cases, hemorrhagic cystitis can be life-threatening; for this reason, any visible blood in the urine is a serious sign that requires medical evaluation.
On the other hand, the most important issues in controlling this condition are “stable circulation and vital signs” and “making sure the bladder is draining”. Therefore, symptoms that suggest a problem with either of these are warning signs, such as:
Inability to pass urine;
Dizziness;
Pale skin;
Fainting.
People with a history of chemotherapy, radiation therapy, or bone marrow transplant should take symptoms of this condition more seriously and seek care more urgently.
Summary
“Hemorrhagic cystitis” is inflammation of the mucosal lining of the bladder wall and causes bleeding from the bladder, so that the urine color changes clearly (gross hematuria) and may even become life-threatening. This complication often occurs after chemotherapy, radiation therapy, or viral infections, and treatment ranges from simple measures to complex surgeries.
Timely diagnosis plays an important role in preventing serious complications such as kidney failure or bladder rupture and gives the treatment team an opportunity to use the most effective and least invasive methods to control the condition. For this reason, recognizing the warning symptoms of this condition is very important.
Frequently Asked Questions
Actions & related links
Related articles
All articlesWhat Is Polycystic Kidney Disease? (Fetal and Adult PKD)
What is polycystic kidney disease? Learn about inherited ADPKD and ARPKD, fetal and adult symptoms, complications, diagnosis, medicines, surgery, diet, fluids, and prevention-focused care.
What Is a Renal Cortical Cyst? Symptoms, Diagnosis, and Treatment
Renal cortical cyst | Simple vs. complex kidney cysts | Warning symptoms | Diagnosis and treatment | Needle drainage, laparoscopy, medication, and ablation
Kidney Transplant: Cost, Blood Type Compatibility, and Surgical Method
What is kidney transplant? Learn about cost considerations, operation duration and method, diet, who may not be eligible, success rates, isolation precautions, and post-transplant care.
What Is Pyelonephritis? Kidney Infection Symptoms, Diagnosis, and Treatment
What is pyelonephritis? Learn kidney infection symptoms in women, children, men, and pregnancy; diagnosis, antibiotics, treatment, emergency warning signs, and cystitis differences.
Comments
0 comments
No comments yet. Be the first to share your thoughts.